Downloaded 809 times




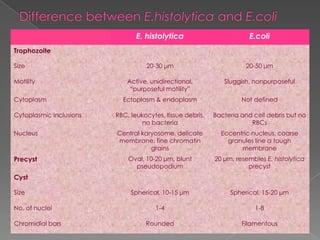

![Luminal amoebicide
Diloxanide furoate
Paromomycin
Diiodohydroxiquin
Liver, gut wall and other tissues
Emetine
Dehydroemetine
Hepatic amoebicide
Chloroquine
Both tissue and intestinal amoebicide (Nitroimidazoles)
Metronidazole [500-800 mg TDS X 5 (5-10) days]
Tinidazole [ 2 gm OD X 1-3 days]
Ornidazole [ 2 gm OD X 1-3 days]
](https://image.slidesharecdn.com/amoebiasislecture-140226093833-phpapp01/85/Amoebiasis-lecture-28-320.jpg)


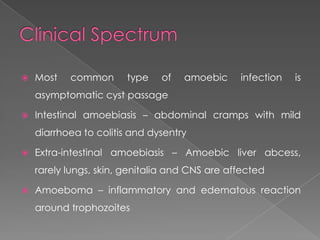
Amoebiasis is caused by the intestinal protozoan Entamoeba histolytica. Most infections are asymptomatic, but 10% can cause a spectrum of clinical syndromes ranging from asymptomatic to dysentery to liver and other organ abscesses. Transmission occurs through the fecal-oral route via contaminated food, water, or direct person-to-person contact. Diagnosis involves microscopic identification of trophozoites in stool or abscess samples and serologic detection of antibodies. Treatment depends on the infection site and involves luminal amoebicides for intestinal infection and tissue amoebicides like metronidazole for extra-intestinal infections such as liver abscesses.






















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


