Downloaded 334 times
![Answer : taksotsubocardiomyopathyThe ECG findings are often confused with those found during an acute anterior wall myocardial infarction.Itclassically mimics ST-segment elevation myocardial infarction, and is characterised by acute onset of transient ventricular apical wall motion abnormalities (ballooning) accompanied by chest pain, dyspnea, ST-segment elevation, T-wave inversion or QT-interval prolongation on ECG. Elevation of myocardial enzymes is moderate at worst and there is absence of significant coronary artery disease.[1]](https://image.slidesharecdn.com/ecgquiz-110527065318-phpapp01/75/Ecg-quiz-15-2048.jpg)
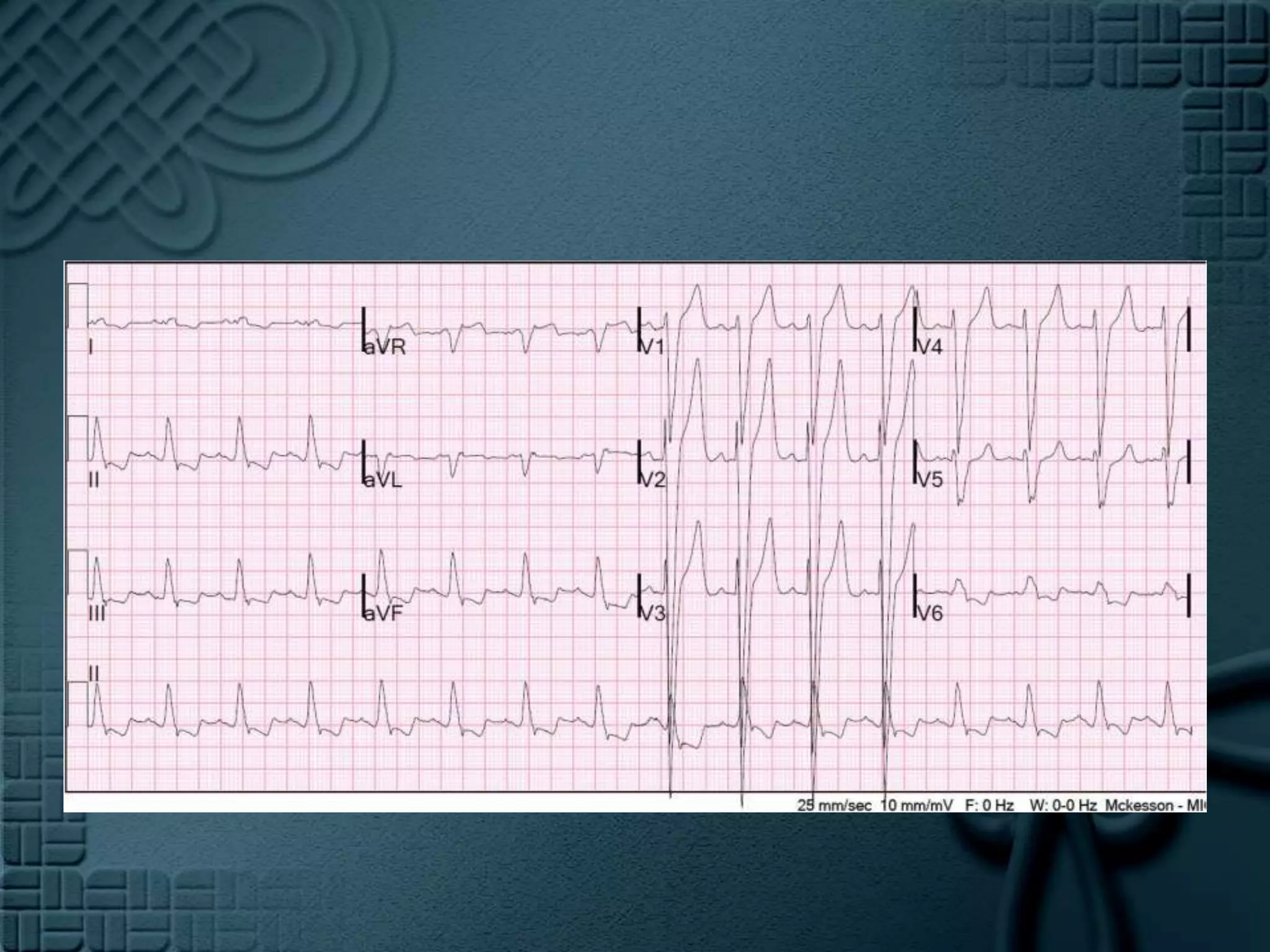
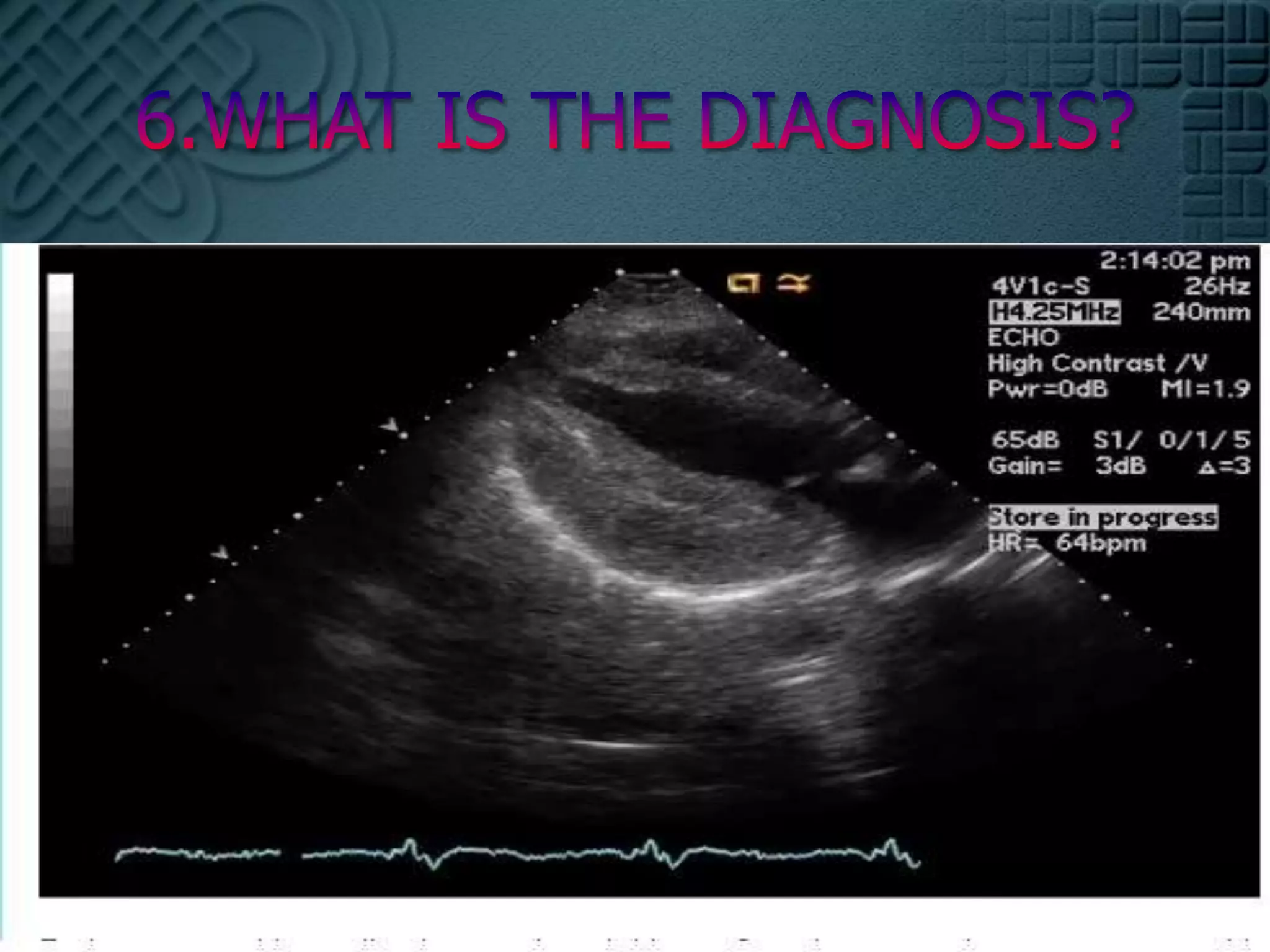

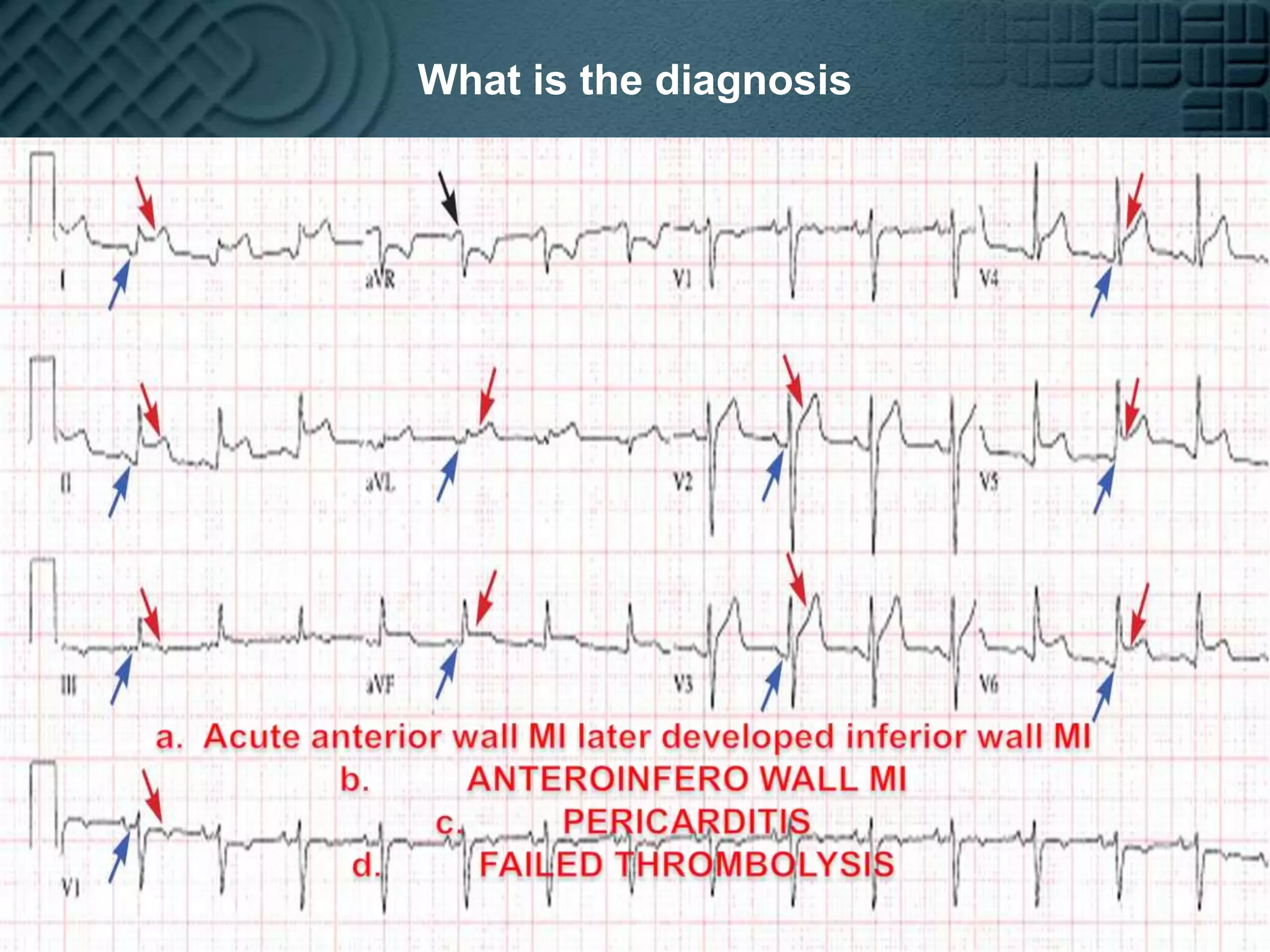
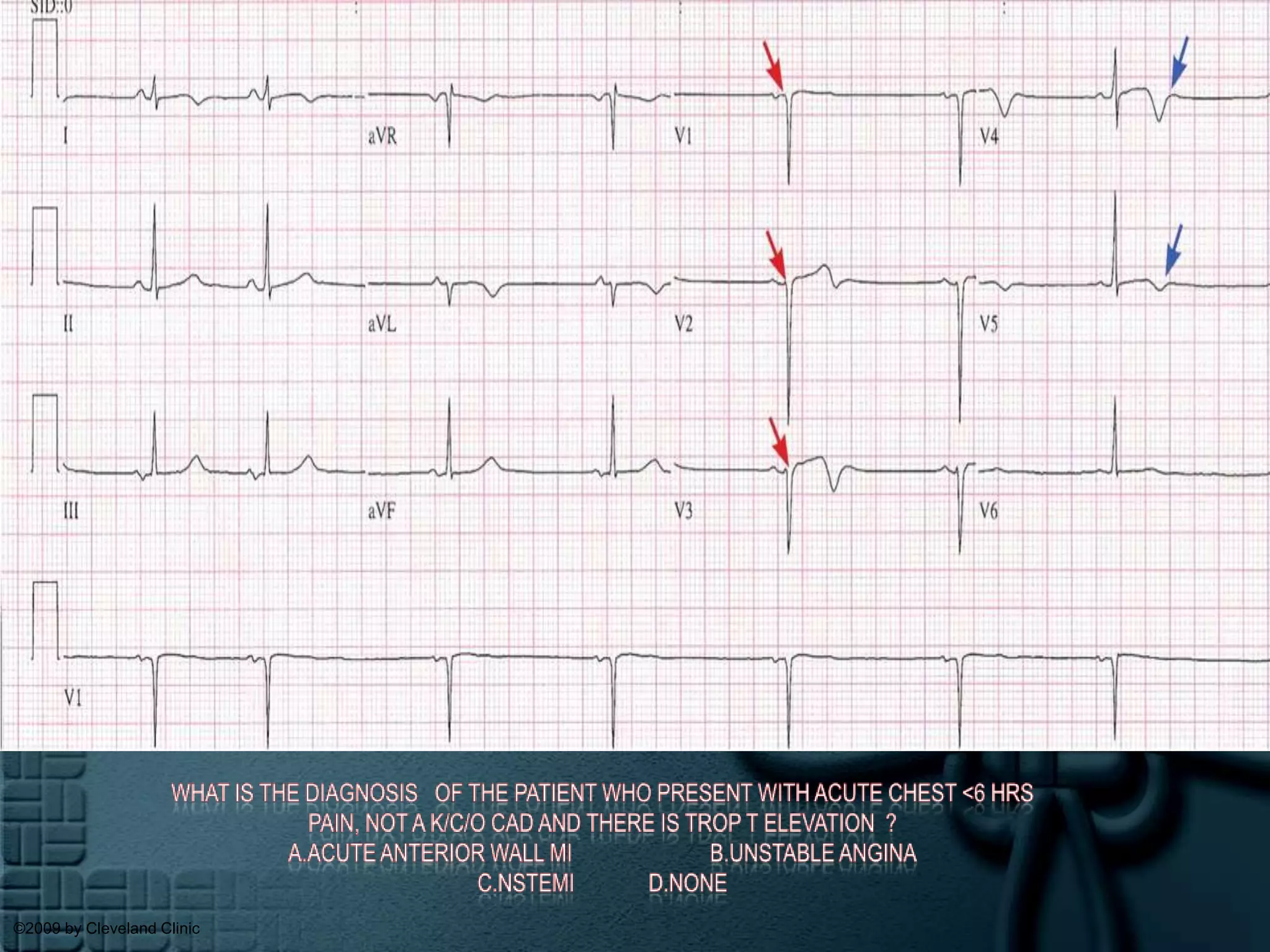
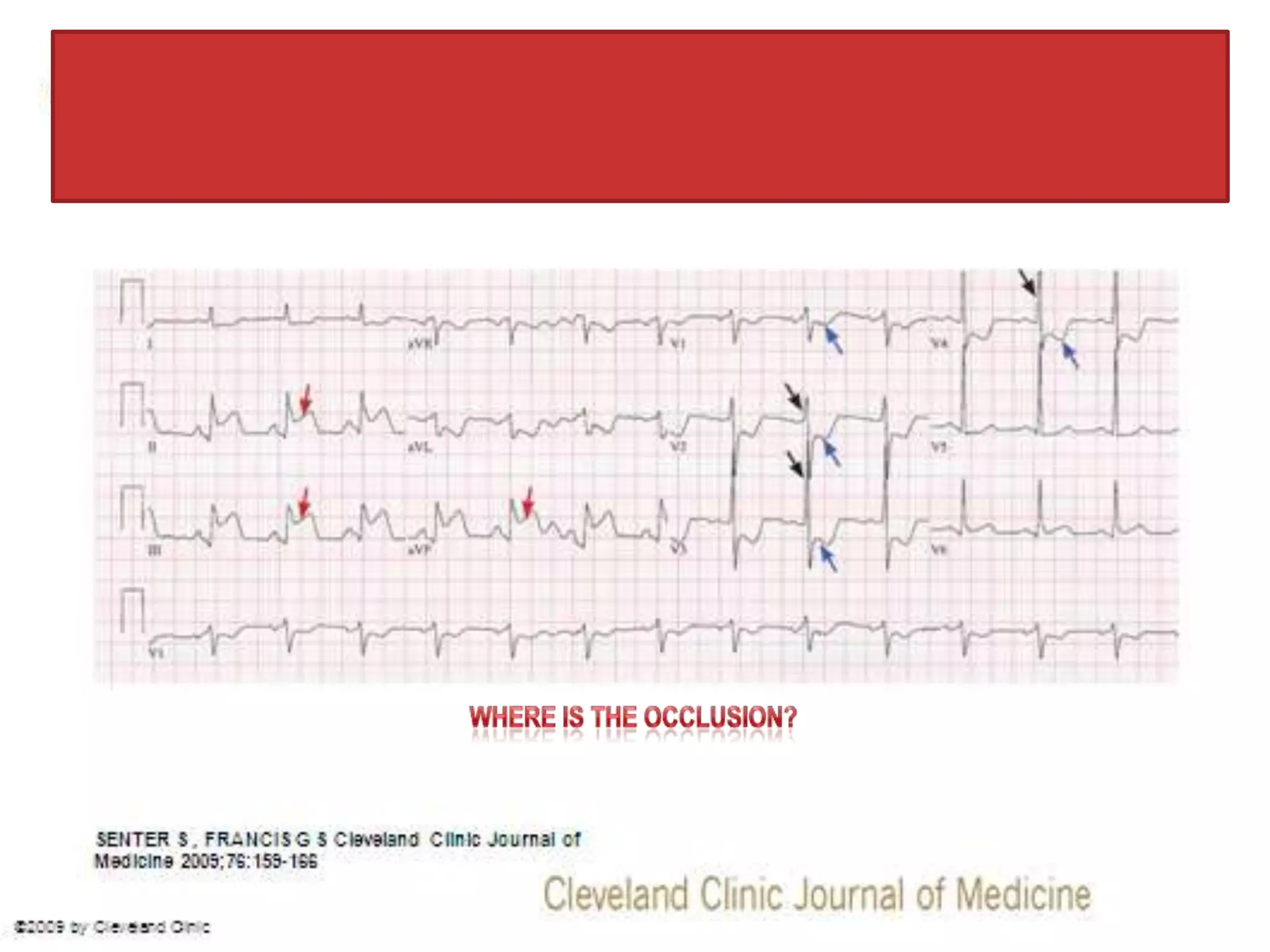
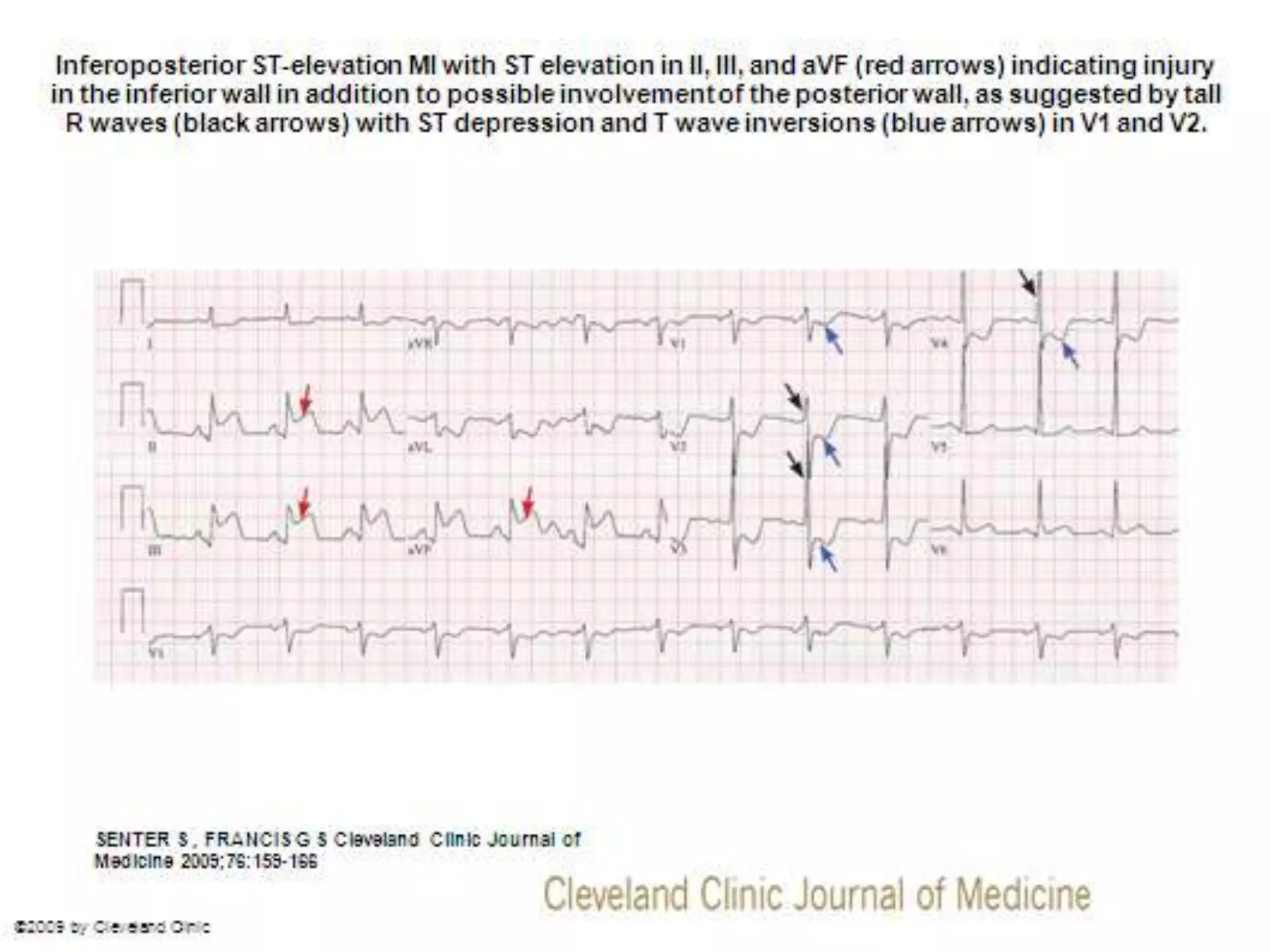
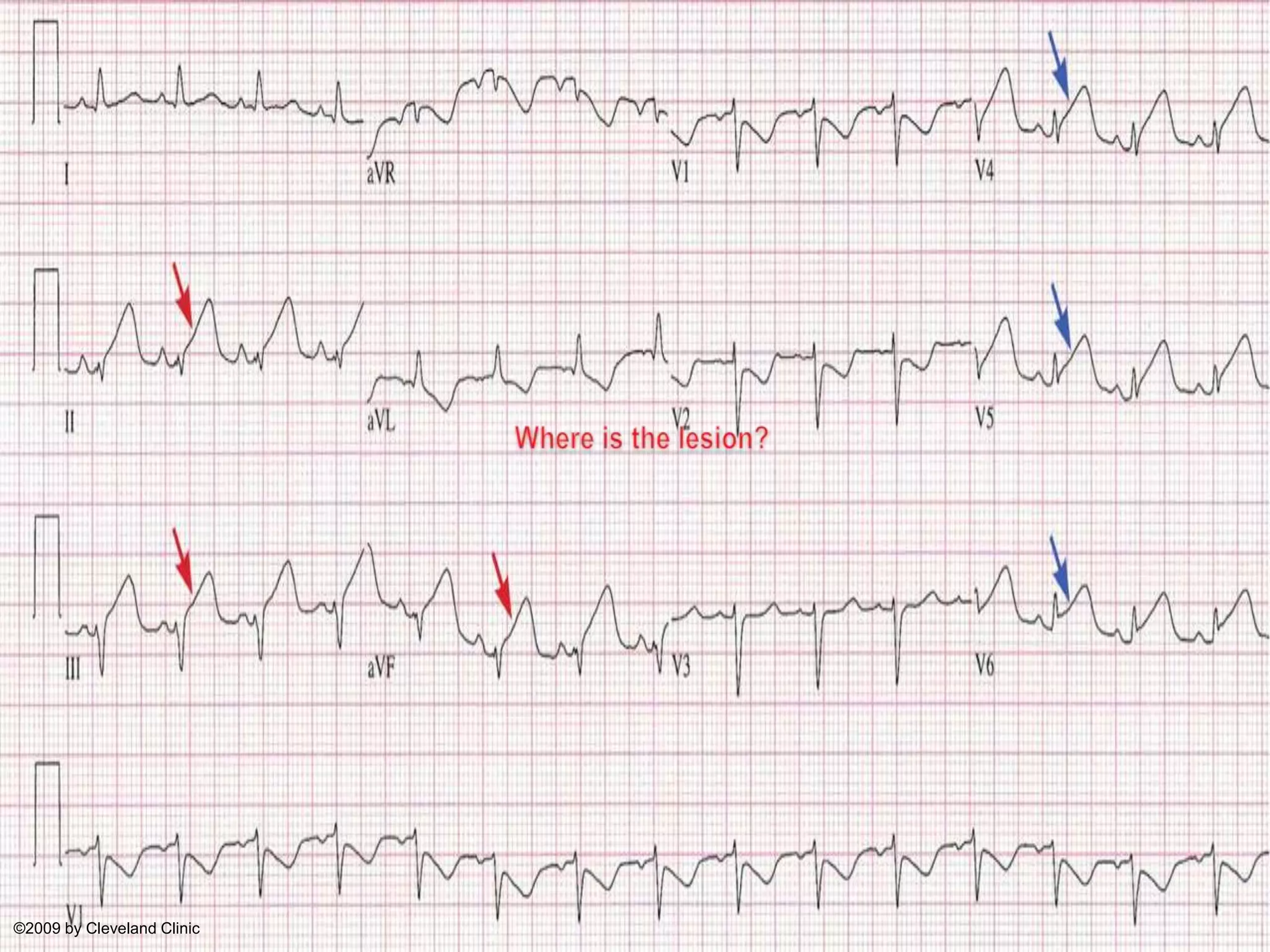
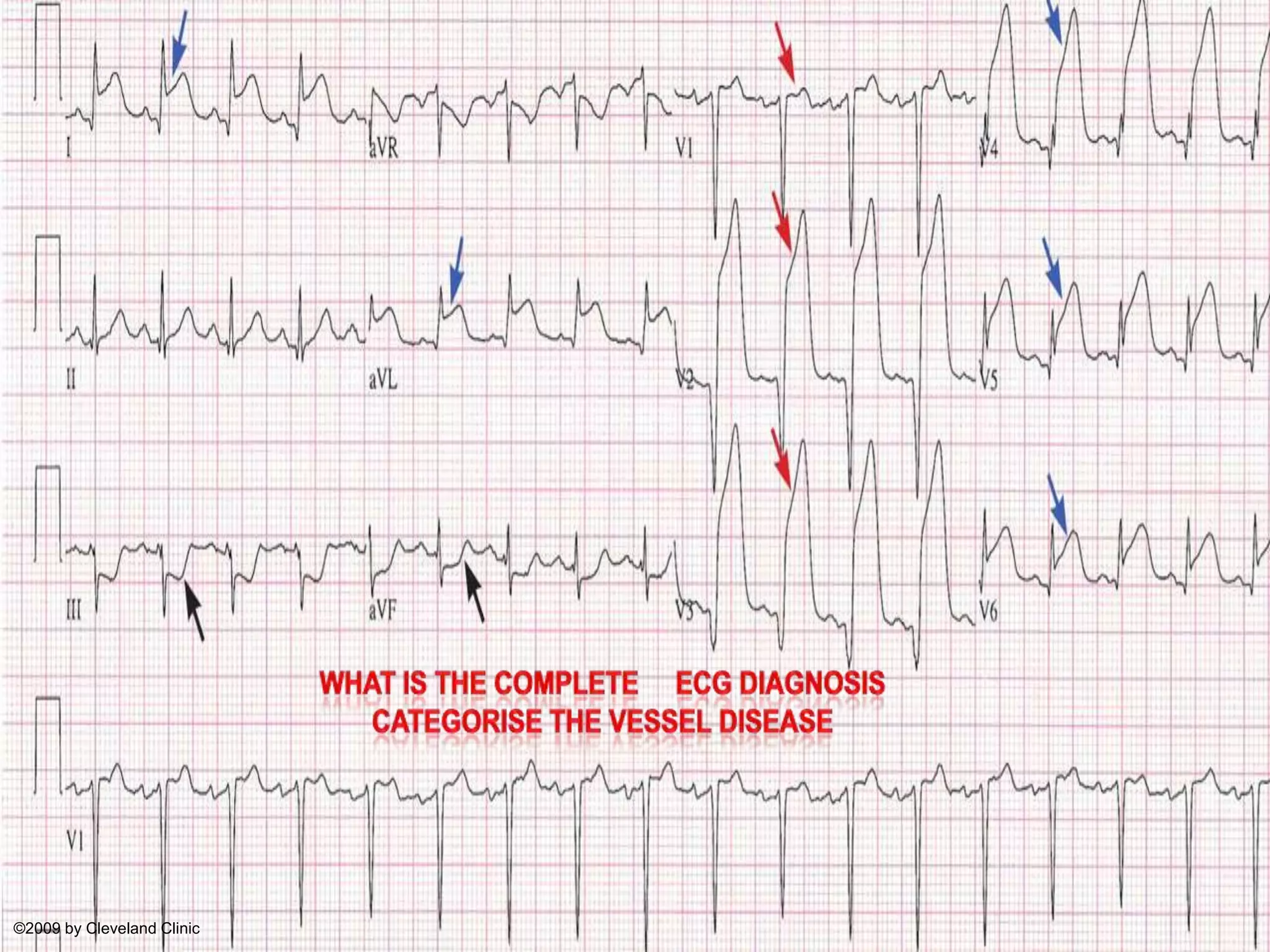
This document contains an ECG quiz that tests the reader's ability to interpret electrocardiograms and diagnose cardiac conditions. It includes 10 multiple choice questions about various ECG readings showing conditions like acute myocardial infarction in different areas of the heart, pericarditis, effects of thrombolysis, and more. The questions aim to evaluate the reader's skill in locating areas of injury, categorizing vessel disease, differentiating disease mimics, and assessing risk of heart block.























































































