Downloaded 456 times



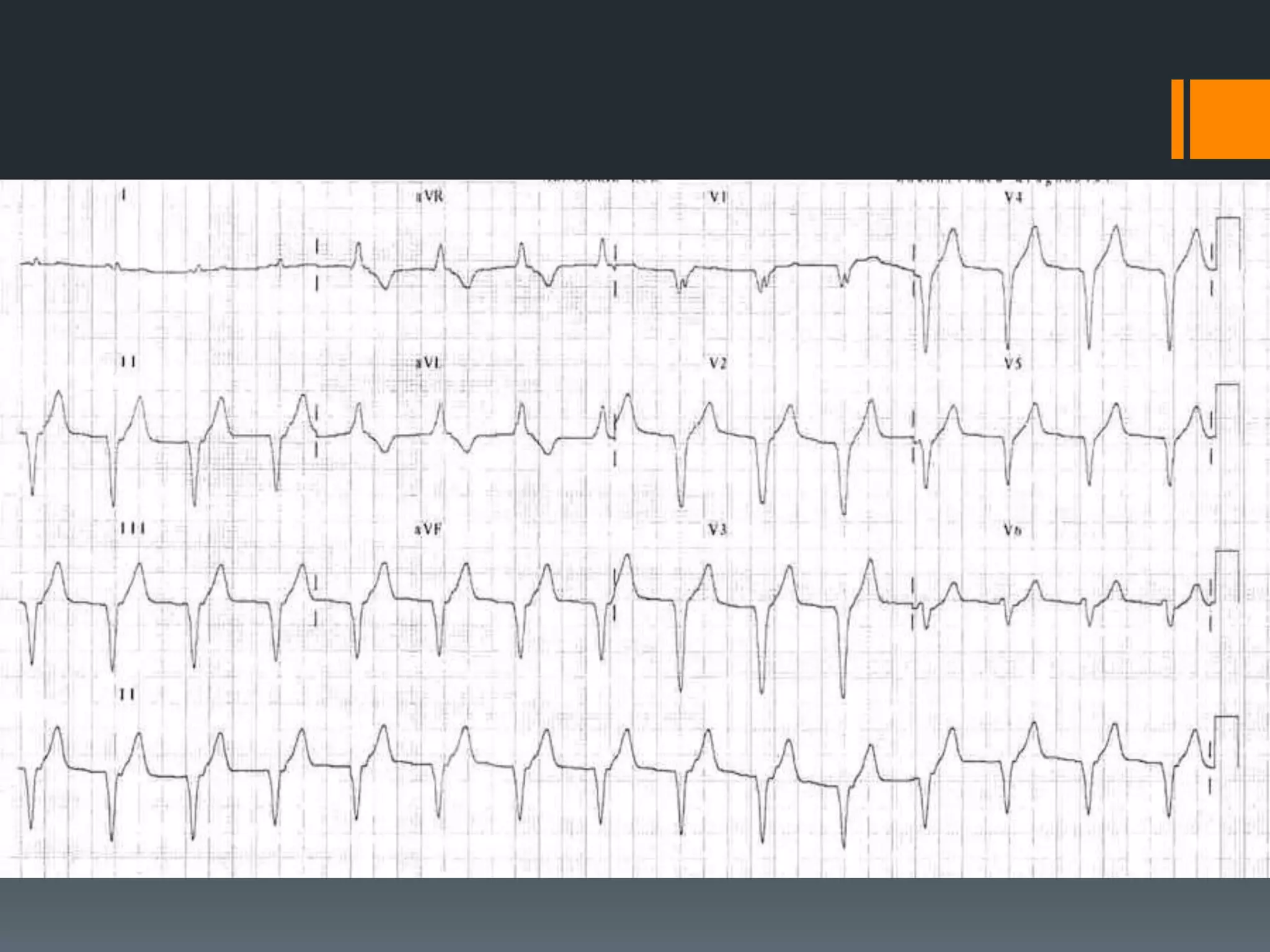












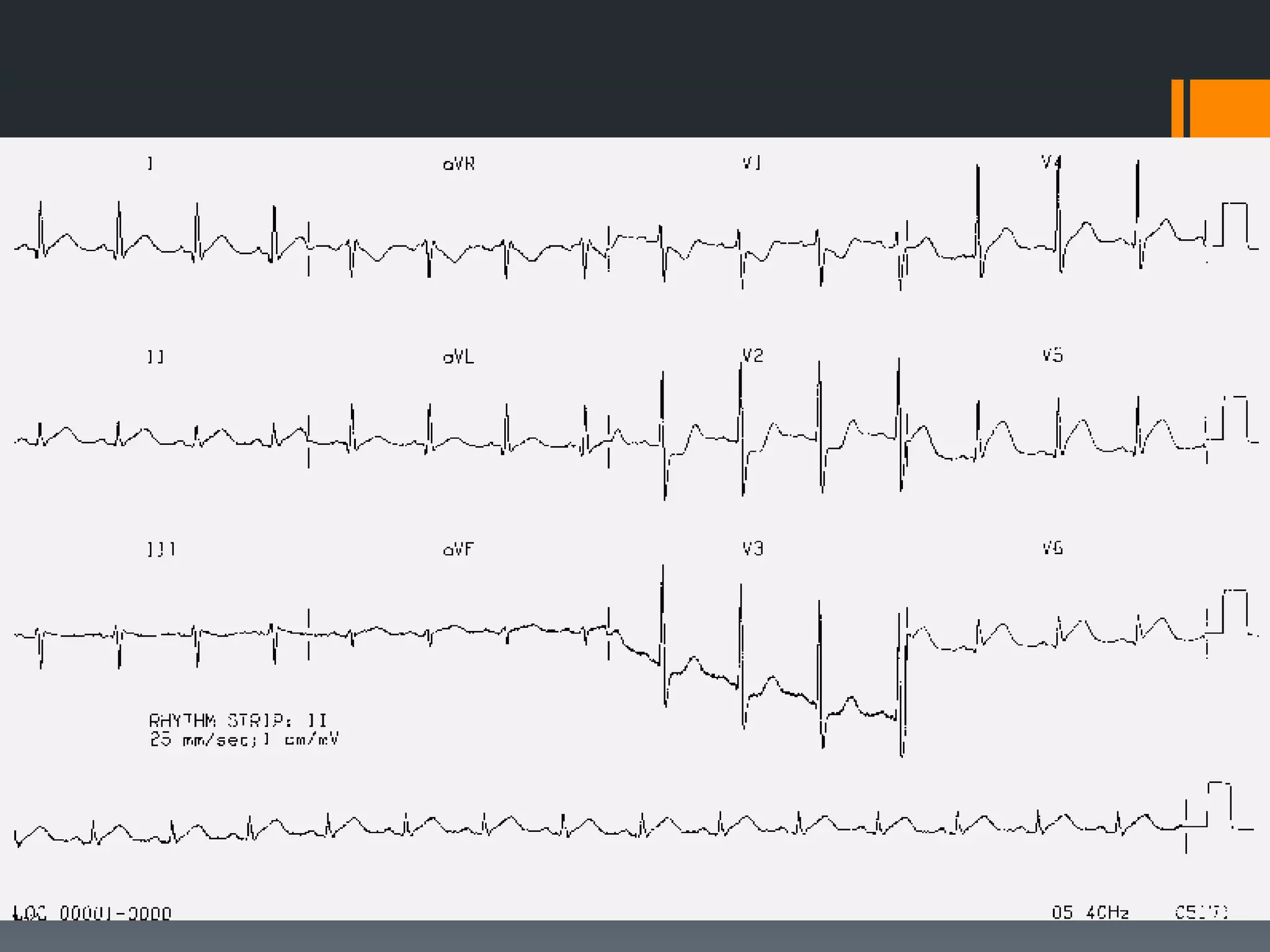

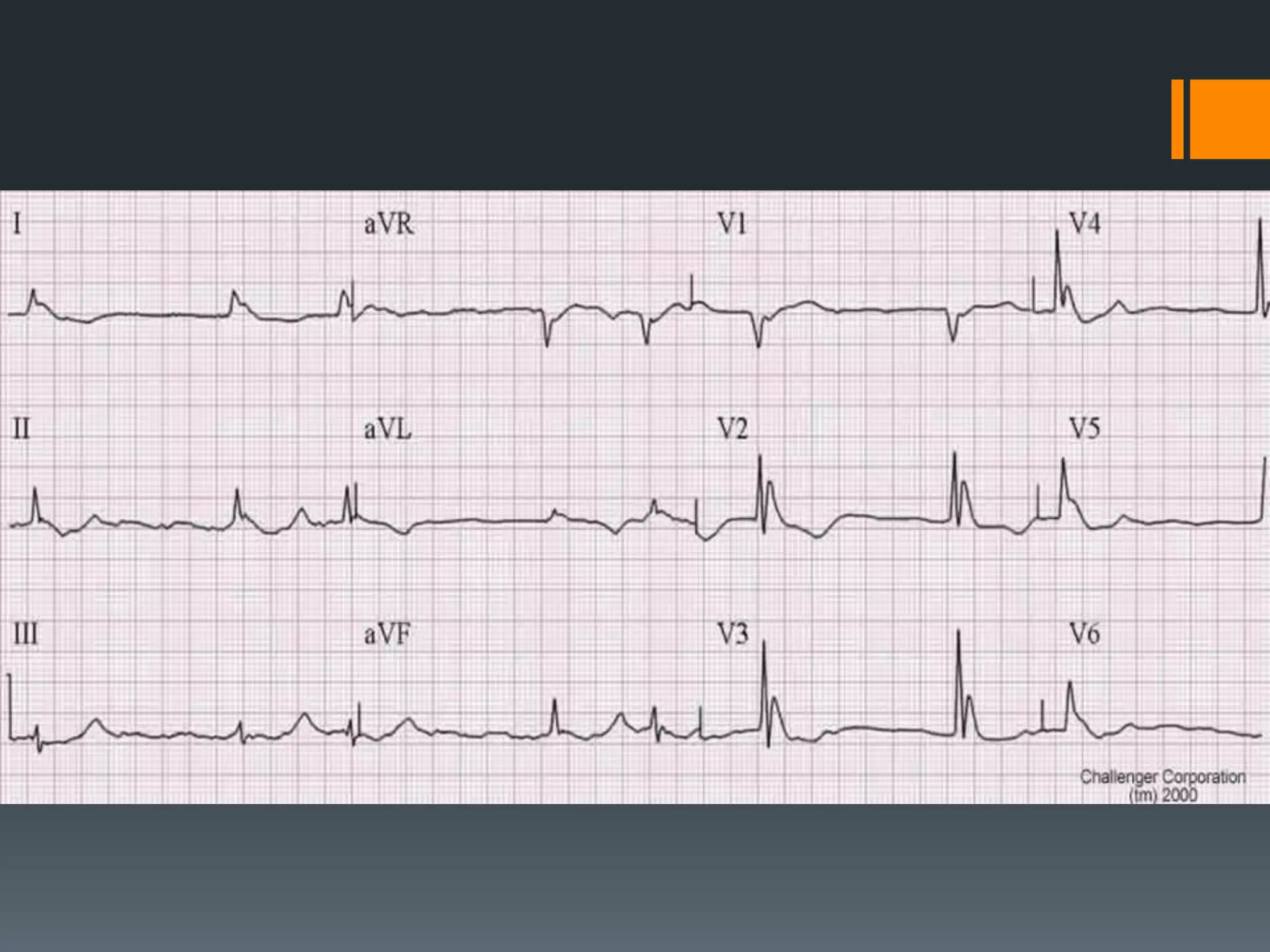

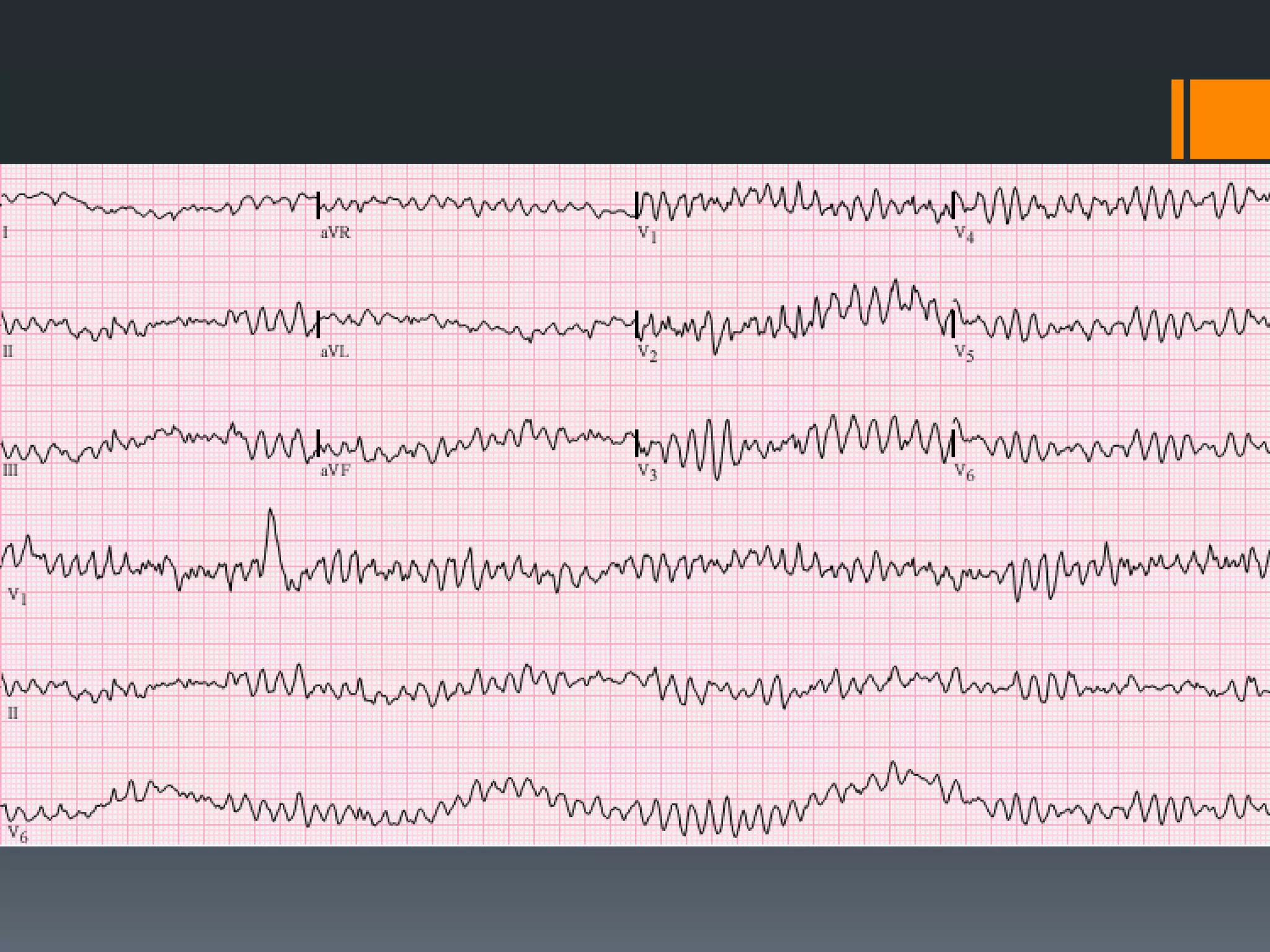




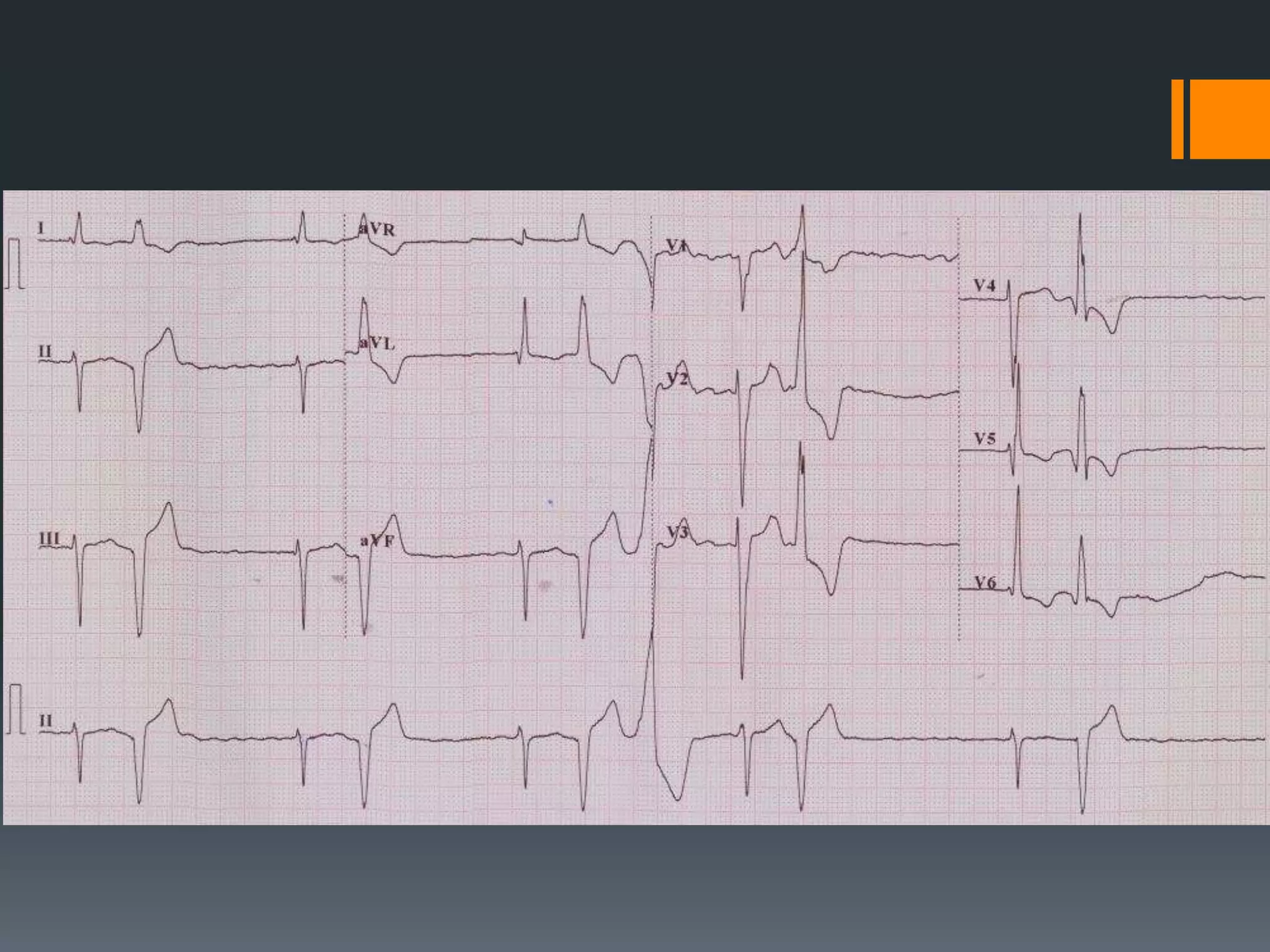














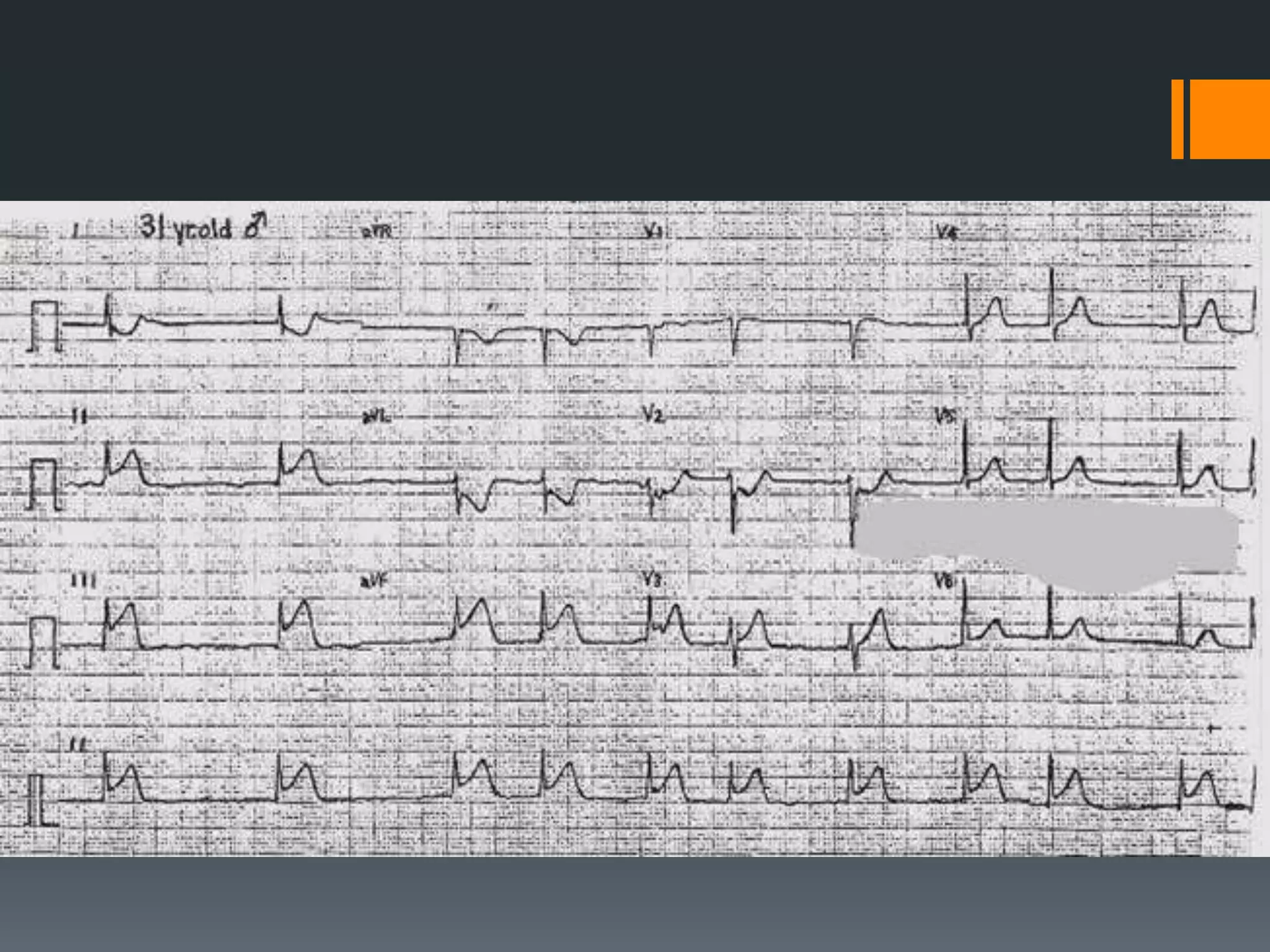

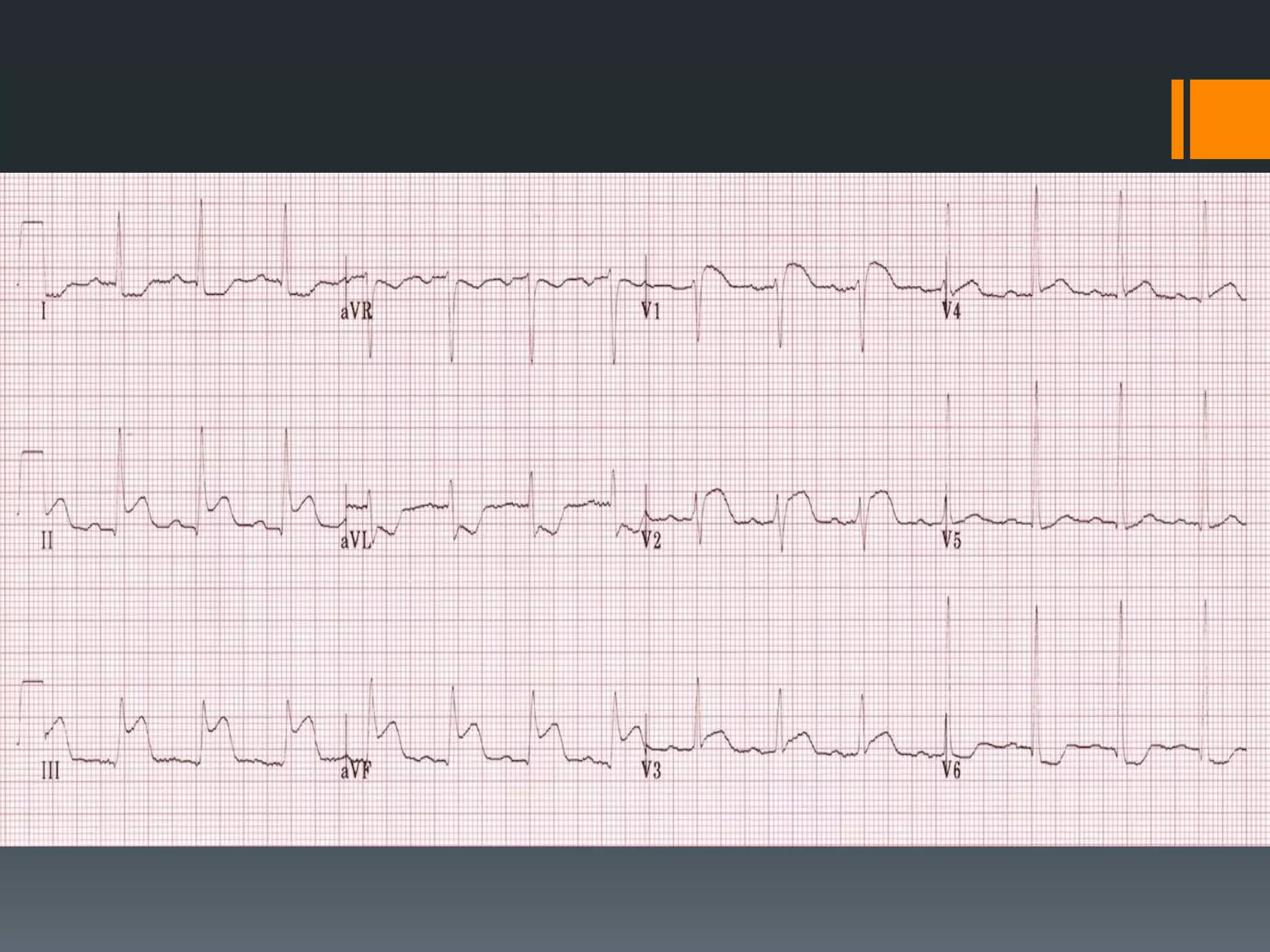

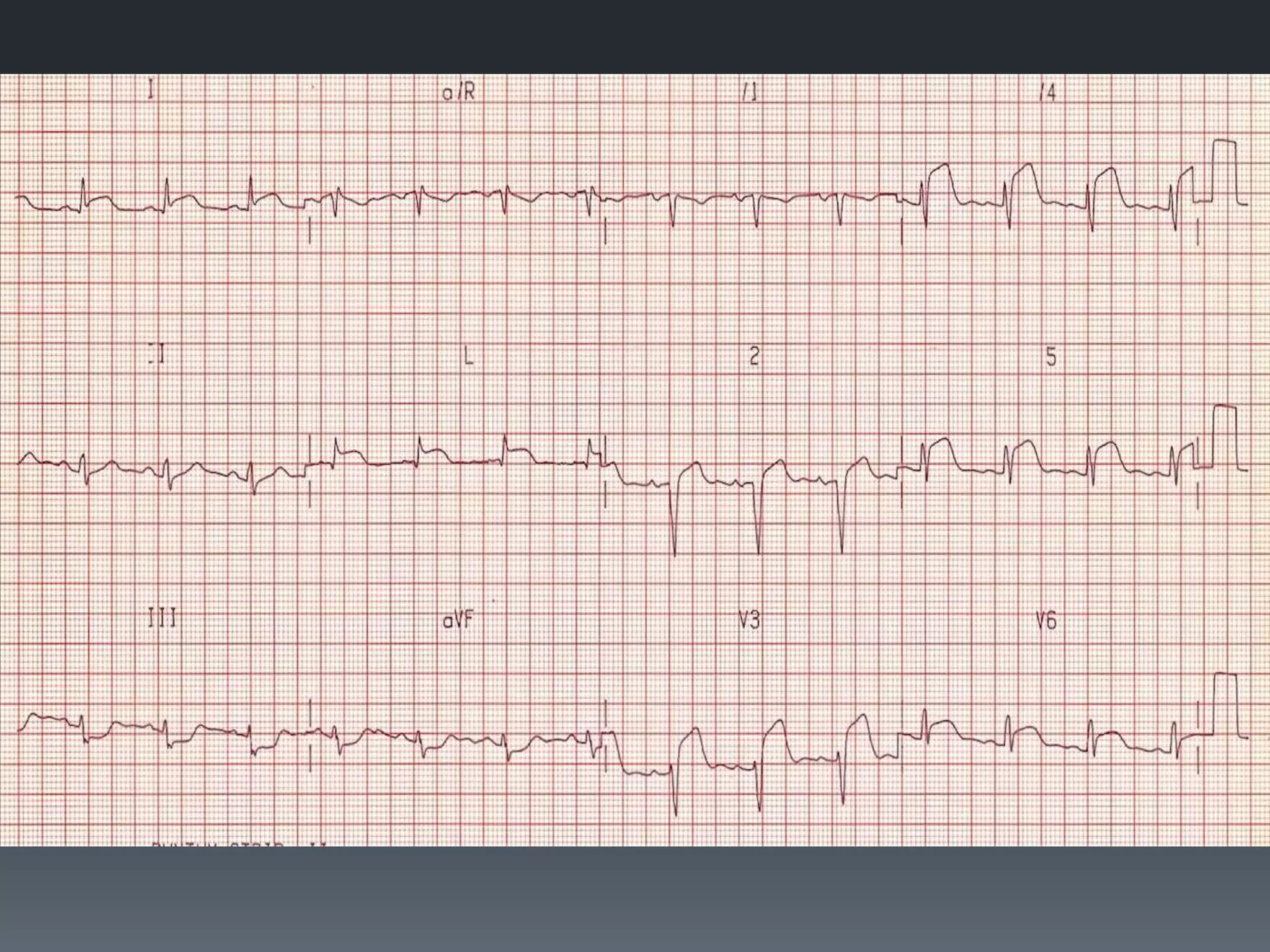

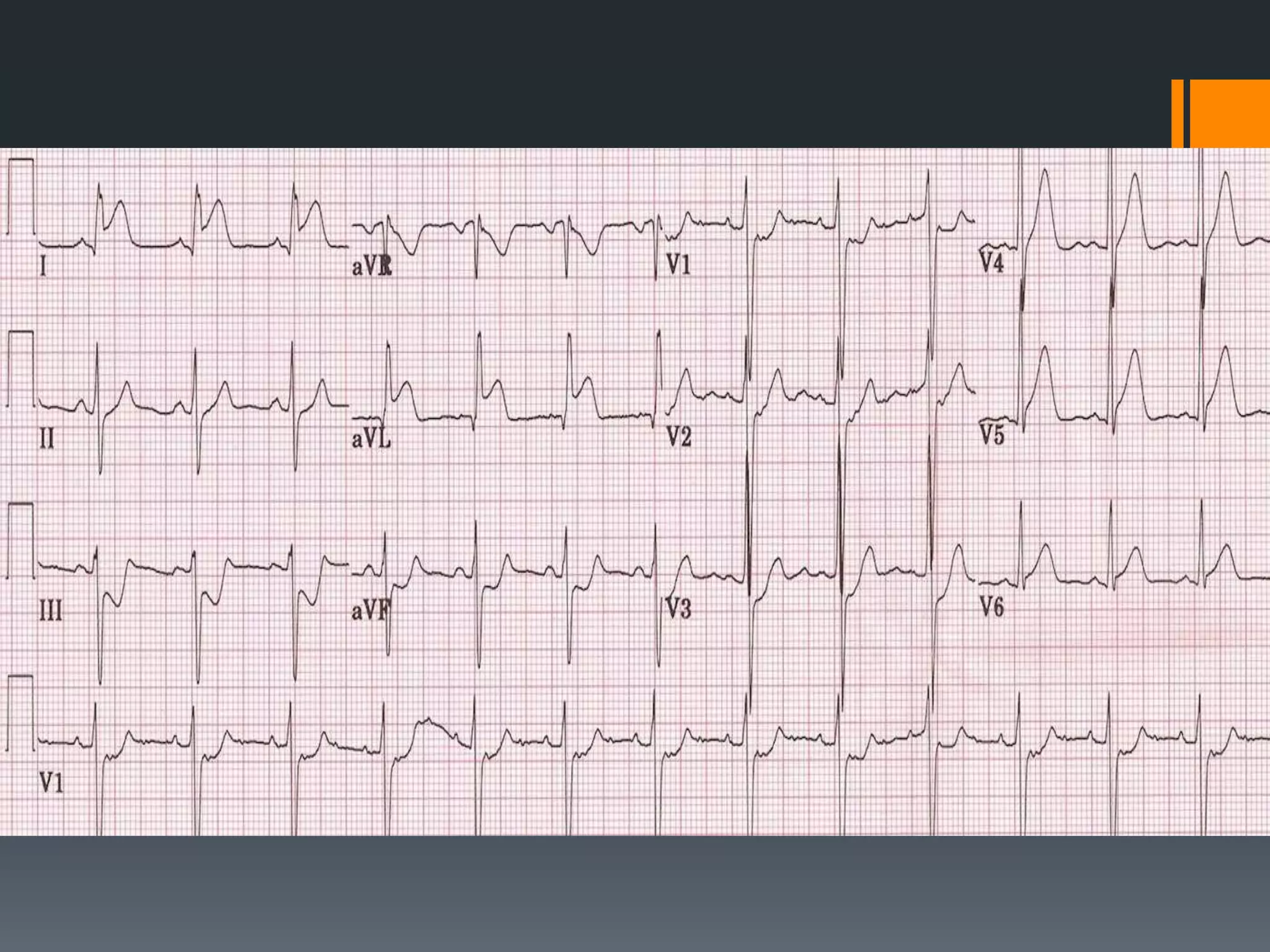











This document provides descriptions of various ECG patterns and cardiac conditions: - It describes limb lead reversal showing a sine wave pattern typical of hyperkalemia. Calcium gluconate and other treatments are recommended. - Accelerated idioventricular rhythm is defined as having a rate between 50-100 bpm and being a type of slow ventricular tachycardia that does not typically require treatment. - Atrial flutter with a 4:1 conduction is described as typical or atypical, with atypical often occurring after surgeries. Atrial flutter can be cardioverted with the least amount of energy. - Several other conditions are briefly defined such as complete heart block, dextro











































































































