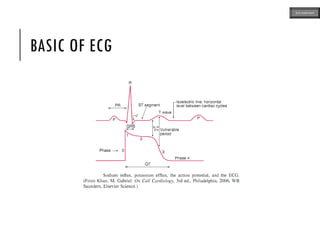
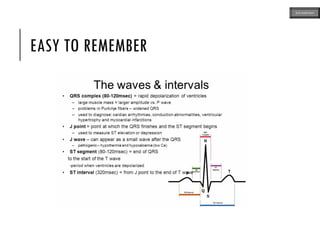
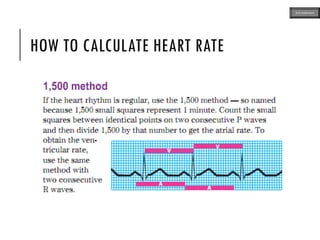
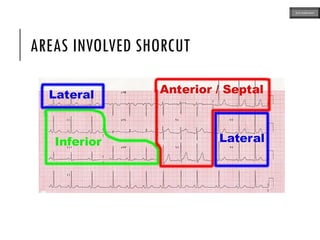
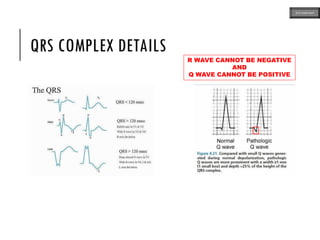
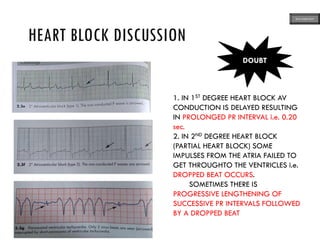
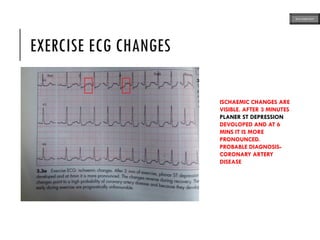
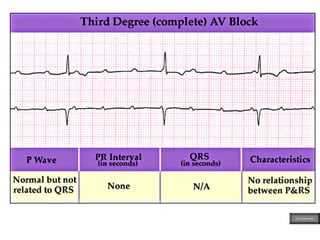
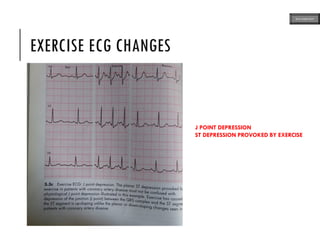
This document provides an overview of ECG samples and diagnosis for medical students. It discusses the basics of ECG interpretation, normal sinus rhythm, intervals, waveforms, abnormalities, myocardial infarction, bundle branch blocks, ventricular hypertrophy, atrial fibrillation, and more. Examples of various abnormal ECG patterns are presented along with explanations. Sources include textbooks and online resources for ECG learning. The document is intended for educational presentation purposes.