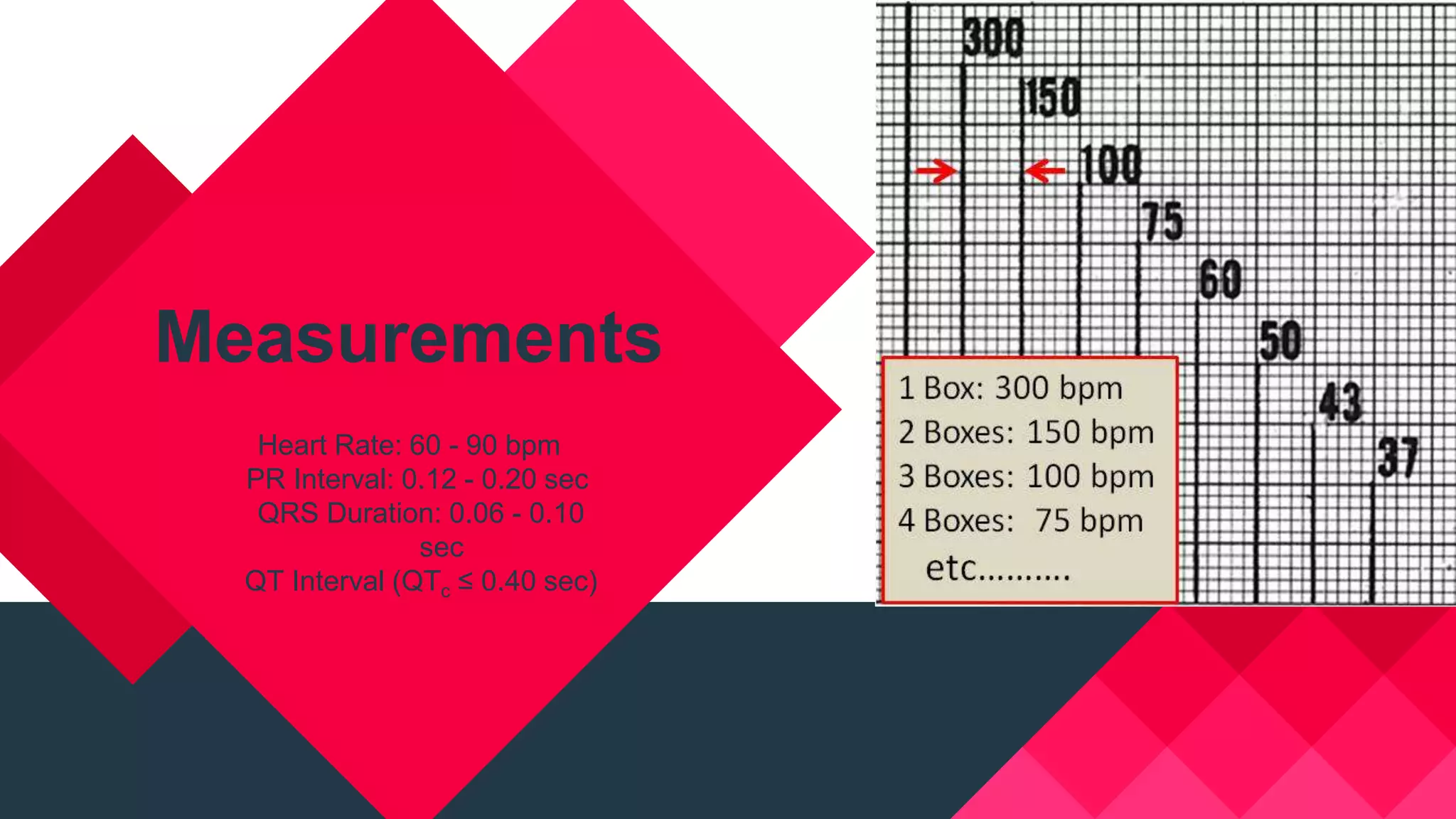













This document describes the normal characteristics of an electrocardiogram (ECG). It outlines normal measurements for heart rate, intervals, and rhythms. It then discusses the normal patterns for P waves, QRS complexes, ST segments, T waves, and U waves in various leads. Key normal findings include upright P waves, QRS duration under 0.10 seconds, mostly positive QRS in leads I and II, ascending R wave and descending S wave in precordial leads, and asymmetrical or smooth ST-T waveform. The document provides details on normal variations and definitions to understand a normal ECG tracing.