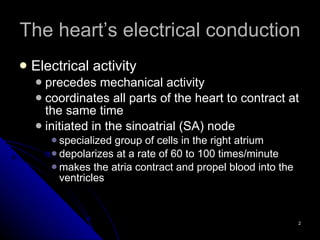
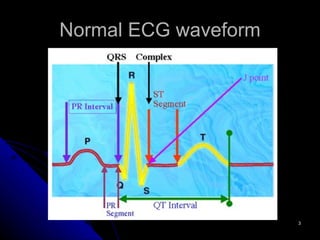
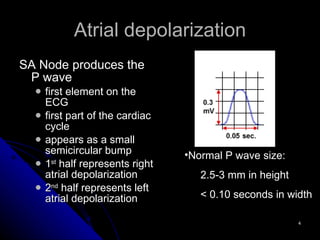
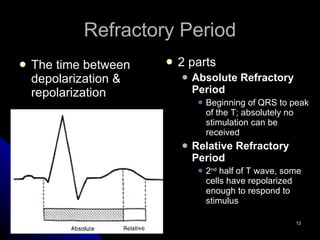
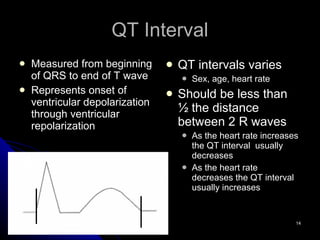
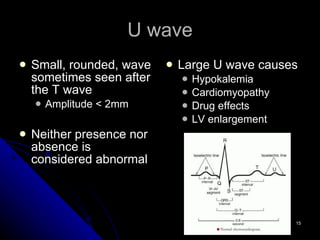
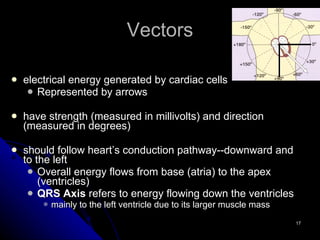
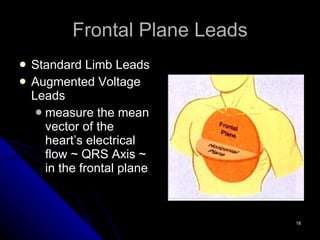
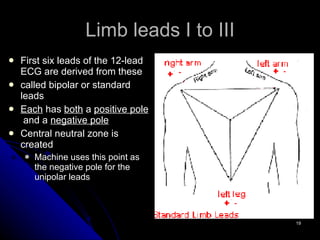
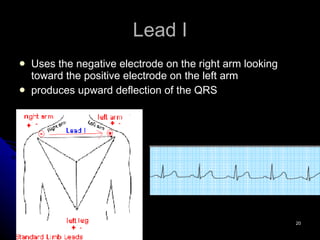
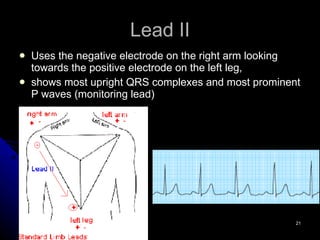
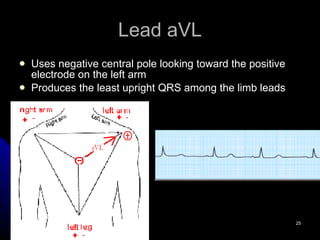
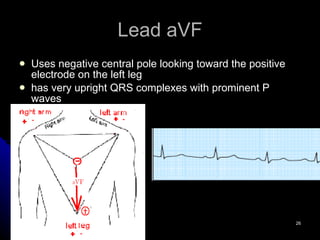
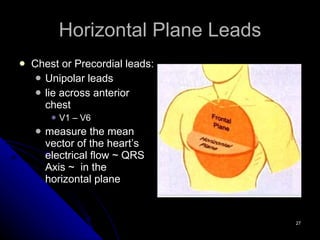
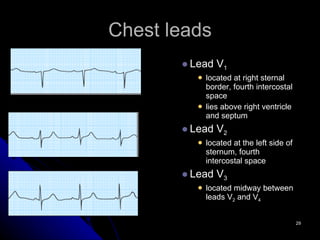
The 12-lead ECG provides important information about the heart's electrical activity. It begins with atrial depolarization seen as the P wave, followed by ventricular depolarization in the QRS complex. The ST segment and T wave represent ventricular repolarization. Each of the 12 leads views the heart from a different angle, with the standard limb leads in the frontal plane and the chest leads in the horizontal plane. Together they allow clinicians to determine the heart's rate, rhythm, and axis.