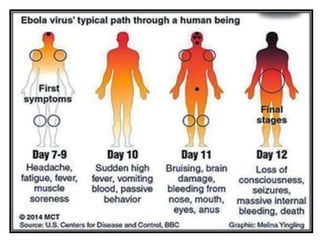
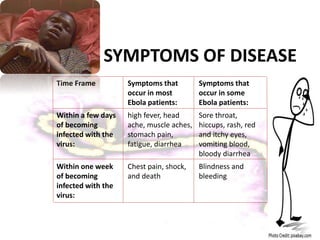
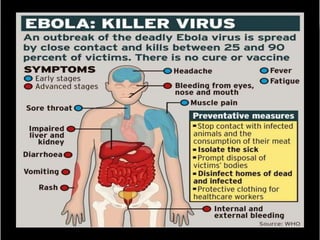
The document provides information on Ebola virus, including its history, outbreaks, transmission, symptoms, diagnosis and potential treatments. It discusses how Ebola was first identified in 1976 near the Ebola River in Africa. It causes severe hemorrhagic fever in humans with high mortality. While fruit bats are suspected to be the natural reservoir, transmission occurs between humans via contact with bodily fluids. Current efforts are focused on supportive care and experimental therapies like monoclonal antibodies, antivirals and immunomodulators until a vaccine is developed.