This document discusses cervical cancer, its causes, symptoms, diagnosis, and treatment. Some key points:
- Cervical cancer is the fourth most common cancer in women worldwide and is caused by human papillomavirus (HPV) infection in over 90% of cases.
- Other risk factors include multiple sexual partners, young age of first intercourse, smoking, and a weakened immune system.
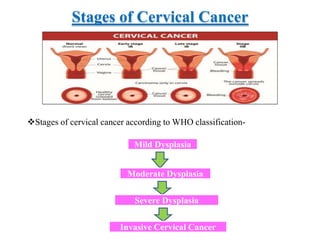
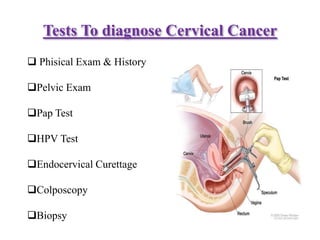
- Symptoms can include abnormal bleeding or discharge. Diagnosis involves exams, Pap tests, HPV tests, biopsies and assessing the cancer stage.
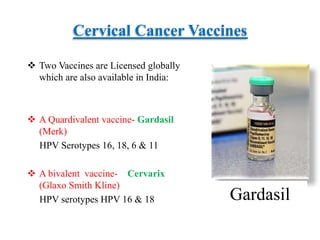
- Cervical cancer is typically treated through surgery, radiation therapy, chemotherapy, or a combination depending on the cancer stage and grade. Vaccines can




















































![H:\Infections In Pregnancy 2008 Cert Day 1[1]](https://cdn.slidesharecdn.com/ss_thumbnails/hinfectionsinpregnancy2008certday11-100304135041-phpapp01-thumbnail.jpg?width=640&height=640&fit=bounds)





















































