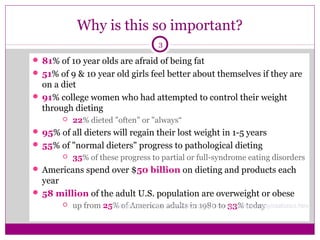
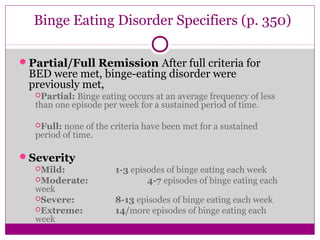
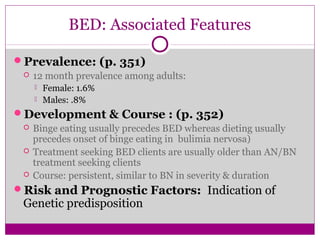
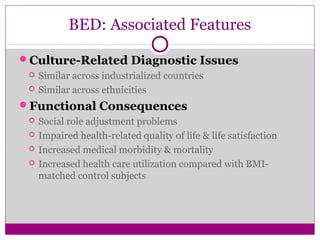
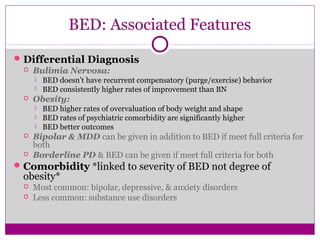
This document discusses eating disorders and related topics. It provides statistics showing that eating disorders are common, especially among young women, and that societal pressures around weight and thinness contribute to their development. The document examines various theories for what causes eating disorders, including genetic, biological, psychological, and socio-cultural factors. Family dynamics and mood disorders are also discussed as potential risk factors. The diagnostic criteria for eating disorders from the DSM-5 such as anorexia nervosa, bulimia nervosa, and binge eating disorder are summarized.