Dissociative (conversion) disorders involve a loss of integration between memories, identity, and bodily control, including various classifications such as dissociative amnesia and dissociative fugue. These disorders can stem from biological, psychodynamic, or behavioral causes and present with symptoms like sensory disruptions, motor disturbances, and altered awareness. Treatment options include behavioral therapy, psychotherapy, and limited drug therapy, focusing on addressing psychological rather than physical causes.


![CLASSIFICATION
• F44.0 Dissociative amnesia
• F44.1 Dissociative fugue
• F44.2 Dissociative stupor
• F44.3 Trance and possession disorders
• F44.4 Dissociative motor disorders
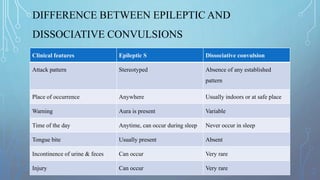
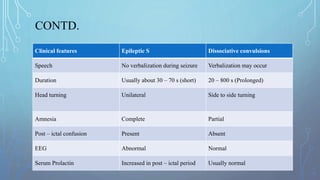
• F44.5 Dissociative convulsions
• F44.6 Dissociative anesthesia and sensory loss
• F44.7 Mixed dissociative [conversion] disorders](https://image.slidesharecdn.com/dissociativedisorder-200902140802/85/Dissociative-disorder-3-320.jpg)
![CONTD.
• F44.8 Other dissociative [conversion] disorders
• .80 Ganser's syndrome
• .81 Multiple personality disorder
• .82 Transient dissociative [conversion] disorders occurring in childhood and
adolescence
• .88 Other specified dissociative [conversion] disorders
• F44.9 Dissociative [conversion] disorder, unspecified](https://image.slidesharecdn.com/dissociativedisorder-200902140802/85/Dissociative-disorder-4-320.jpg)




















![Dissociative [conversion] disorders](https://cdn.slidesharecdn.com/ss_thumbnails/dissociativeconversiondisorders-150324052824-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)



























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)






