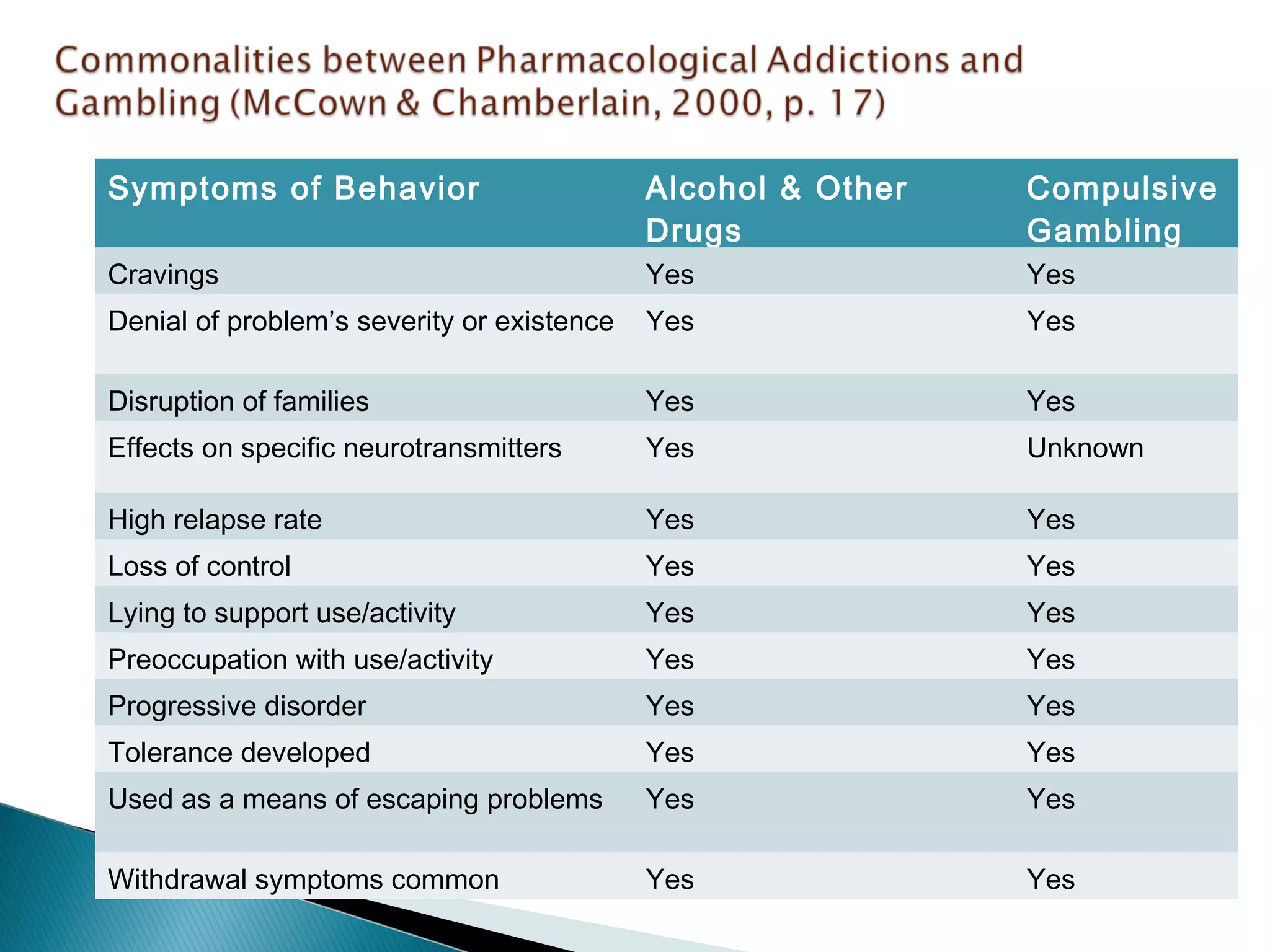
This document discusses compulsive gambling and problem gambling. It defines compulsive gambling as gambling behavior that violates one's intentions to limit gambling. Problem gambling is defined as gambling behavior that causes disruptions in major life areas or is associated with impaired functioning. Many of the same symptoms are seen in compulsive gambling as in substance use disorders, including denial of the problem, disruption of families, loss of control, and lying. Screening tools and assessments for problem gambling are also discussed.


![ “The risk for self-destructive behavior is higher [in
gambling] than with any other addiction”
(Chamberlain, 2004).
The longer they are able to hide the gambling, the
more problematic it becomes. There are no obvious
signs of intoxication, like substance dependence.
Gambling is non-linear in it’s consequences (may
have a win as they are going through a downward
spiral, where substance addiction consequences
generally progressively get worse.)](https://image.slidesharecdn.com/gamblingusedisorderprocessaddictions-141105130607-conversion-gate01/75/Gambling-use-disorder-process-addictions-40-2048.jpg)