Downloaded 331 times
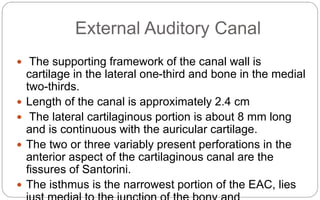
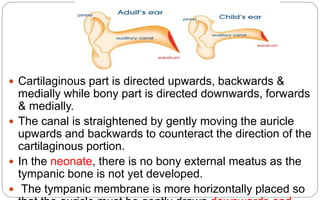







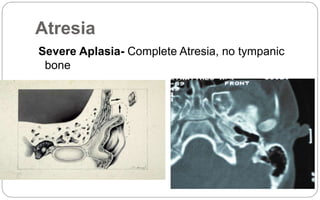
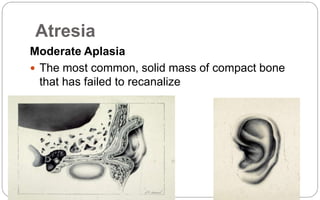















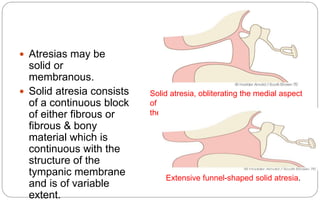
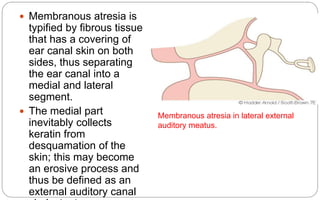

































































The document describes the anatomy and clinical features of the external auditory canal. It discusses the following key points: - The external auditory canal has both cartilaginous and bony portions, with the bony portion making up the medial two-thirds. It is lined by skin that grows obliquely to prevent blockage. - Aural atresia is the absence or closure of the external auditory canal. It can be congenital or acquired. Types include minor, moderate, and severe aplasia. Surgery aims to reconstruct the canal but has risks. - Acquired atresia is due to inflammation, trauma, burns or previous ear surgery. It can be solid from





























































































