Downloaded 85 times





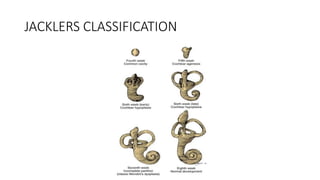


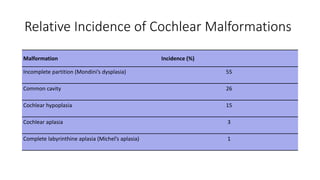





The document discusses various inner ear malformations, including their classification, incidence, and implications for cochlear implantation. It highlights specific malformations such as complete and partial membranous labyrinthine dysplasia, cochleosaccular dysplasia, and incomplete partition, along with their associated challenges and outcomes for hearing interventions. Additionally, it describes conditions like enlargement of the vestibular aqueduct and hearing loss syndromes, stressing the importance of precise diagnostic approaches such as MRI and CT scans.



































































