Download to read offline
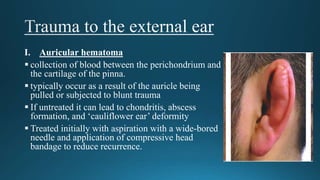


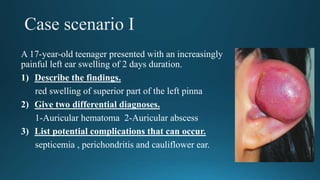

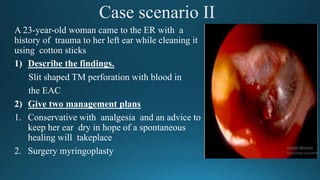


1) The document discusses various traumatic ear injuries including auricular hematoma, lacerations, avulsions, burns, frostbite, tympanic membrane perforations, ossicular injuries, and temporal bone fractures. 2) It provides details on the causes, clinical presentations, investigations, and management approaches for each type of injury. Conservative and surgical treatment options are described. 3) Complications of untreated injuries like auricular hematoma are discussed, which can include chondritis, abscess formation, and deformity. Proper treatment and follow-up are emphasized to prevent long-term issues.



































































