Downloaded 87 times
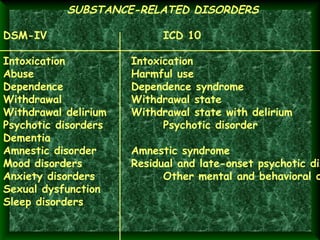




This document discusses substance abuse and provides definitions and classifications of commonly abused substances. It describes substance-related disorders according to the DSM-IV and ICD-10 and covers definitions of key terms like drug, tolerance, withdrawal syndrome, medical use, and non-medical use. The major classes of abused substances discussed include opioids, depressants, tranquilizers, stimulants, hallucinogens, cannabis, inhalants, and cocaine. Signs and symptoms of abuse and withdrawal are outlined for different substance classes. Principles of treatment include detoxification, abstinence, family involvement, screening, and self-help groups.