Downloaded 613 times






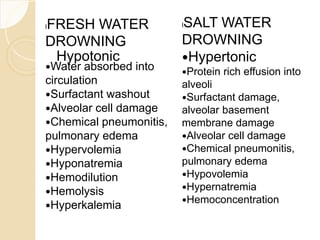
















Drowning is defined as the respiratory impairment resulting from submersion in liquid, with a significant incidence in India and China. The document outlines causes, types, and classifications of drowning, including the dangers faced by different age groups and conditions. It also covers management strategies for near-drowning incidents, emphasizing the importance of prompt medical attention, observation, and various treatment protocols.






















































![Pathophysiology and clinical_features_of_hemolytic_anemia[1]](https://cdn.slidesharecdn.com/ss_thumbnails/pathophysiologyandclinicalfeaturesofhemolyticanemia1-160728175751-thumbnail.jpg?width=640&height=640&fit=bounds)


























