Downloaded 64 times
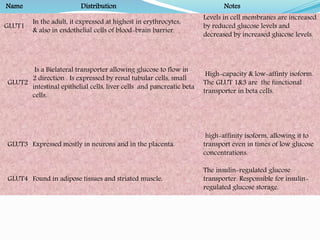



There are 13 glucose transporter proteins (GLUTs) that transport glucose across cell membranes. They are divided into 3 classes. Class I includes GLUT1-4, the most well studied of which are GLUT1, GLUT2, GLUT3 and GLUT4. GLUT1 transports glucose across the blood-brain barrier. GLUT2 acts as a bidirectional transporter in the liver and pancreas. GLUT3 transports glucose into neurons. GLUT4 is the insulin-regulated transporter that transports glucose into muscle and fat cells for storage. Defects in these transporters can lead to diseases like diabetes.




















![White blood cells [wbc]](https://cdn.slidesharecdn.com/ss_thumbnails/whitebloodcellswbc-180530054405-thumbnail.jpg?width=640&height=640&fit=bounds)






















![gluconeogenesis[1].pdf UNDERGRADUATE PROGRAM](https://cdn.slidesharecdn.com/ss_thumbnails/gluconeogenesis1-250505131119-52587b86-thumbnail.jpg?width=640&height=640&fit=bounds)
























![Pathophysiology and clinical_features_of_hemolytic_anemia[1]](https://cdn.slidesharecdn.com/ss_thumbnails/pathophysiologyandclinicalfeaturesofhemolyticanemia1-160728175751-thumbnail.jpg?width=640&height=640&fit=bounds)

























