Downloaded 19 times
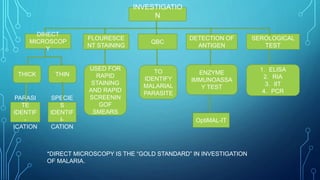
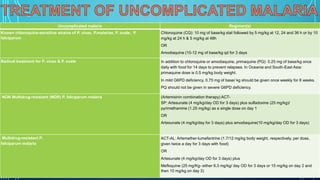
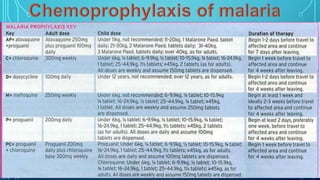


Direct microscopy is the gold standard for investigating malaria. Various serological and molecular tests can also be used to identify the malaria parasite and species. For uncomplicated malaria caused by Plasmodium vivax, P. malariae, P. ovale, or chloroquine-sensitive P. falciparum, treatment options include chloroquine or amodiaquine. For P. vivax and P. ovale infections, primaquine is also given to prevent relapses. Multidrug-resistant P. falciparum is treated with artemisinin combination therapy. For severe P. falciparum malaria, parenteral artesunate, artemether or quinine can be given









































































![Pathophysiology and clinical_features_of_hemolytic_anemia[1]](https://cdn.slidesharecdn.com/ss_thumbnails/pathophysiologyandclinicalfeaturesofhemolyticanemia1-160728175751-thumbnail.jpg?width=640&height=640&fit=bounds)

























