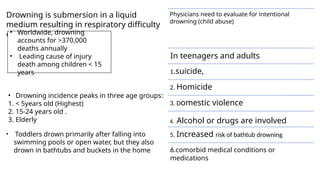
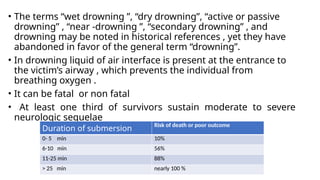
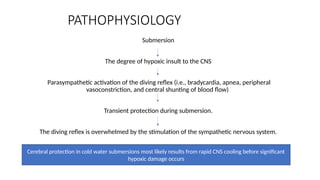
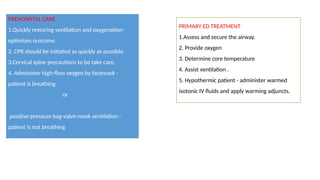
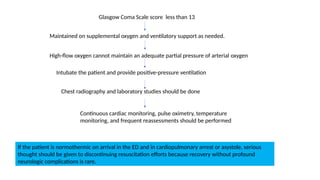
Drowning results in respiratory distress or arrest and is responsible for over 370,000 deaths annually, particularly affecting children under 15, individuals aged 15-24, and the elderly. Prognostic factors such as the duration of submersion and hypoxia greatly influence survival outcomes, with common complications including neurological damage and cardiac arrest. Effective prehospital and emergency care, including immediate CPR and oxygenation, are crucial for optimizing recovery chances.