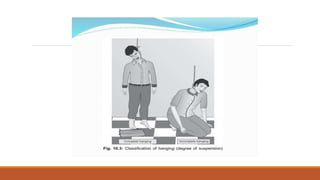
Hanging is a form of asphyxia caused by suspension of the body by a ligature around the neck. It can be complete or partial depending on degree of suspension. The ligature mark is the most important sign and depends on factors like composition, width, and position of the knot. Death is usually due to asphyxia, venous congestion, or cerebral ischemia. In judicial hanging, placement of the knot below the chin and a drop is designed to cause neck fracture or brainstem rupture for a quick death. Key signs include the ligature mark, petechiae, internal carotid artery injuries, and fractures of the hyoid bone or cervical vertebrae.