Downloaded 618 times











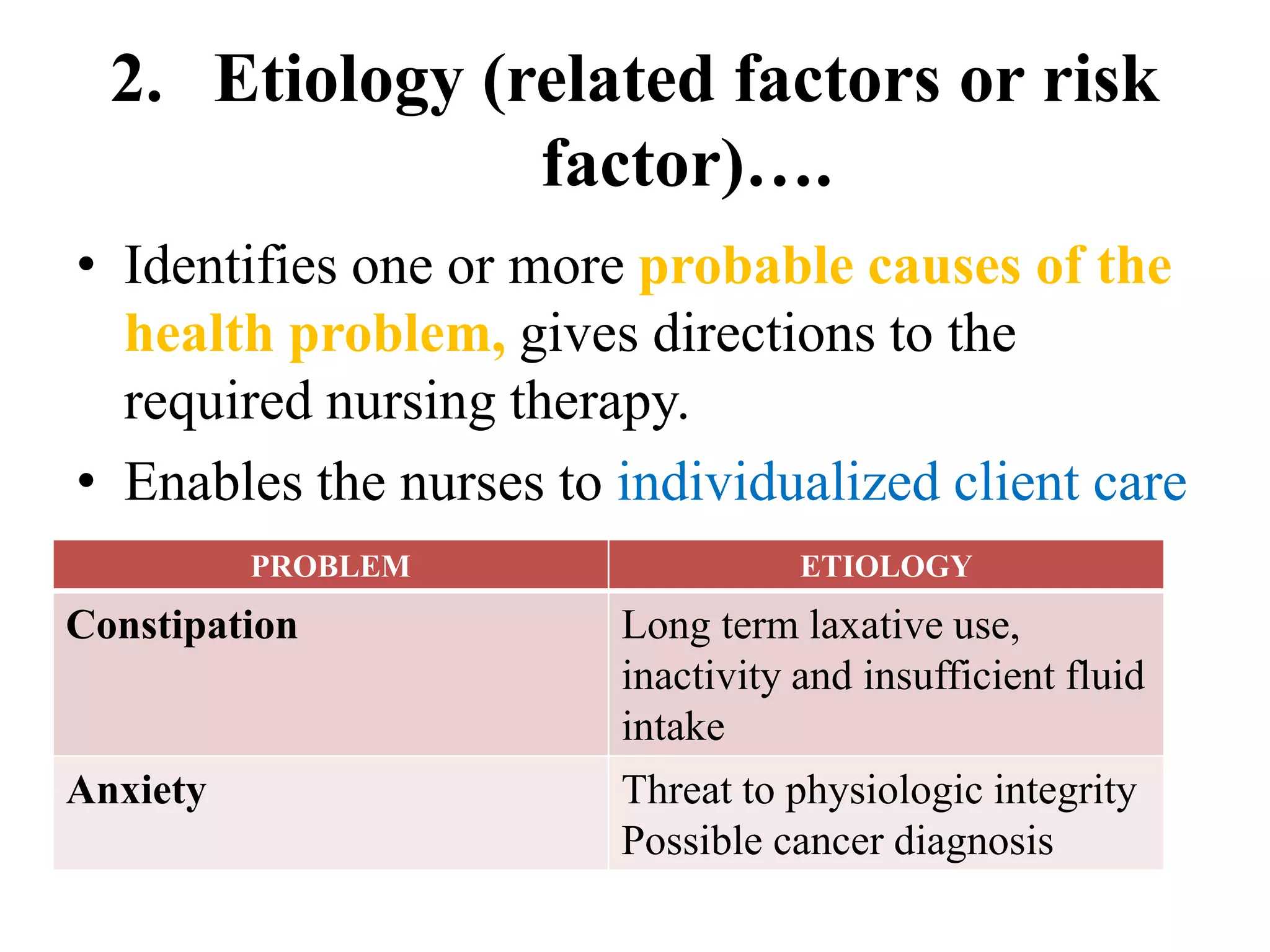







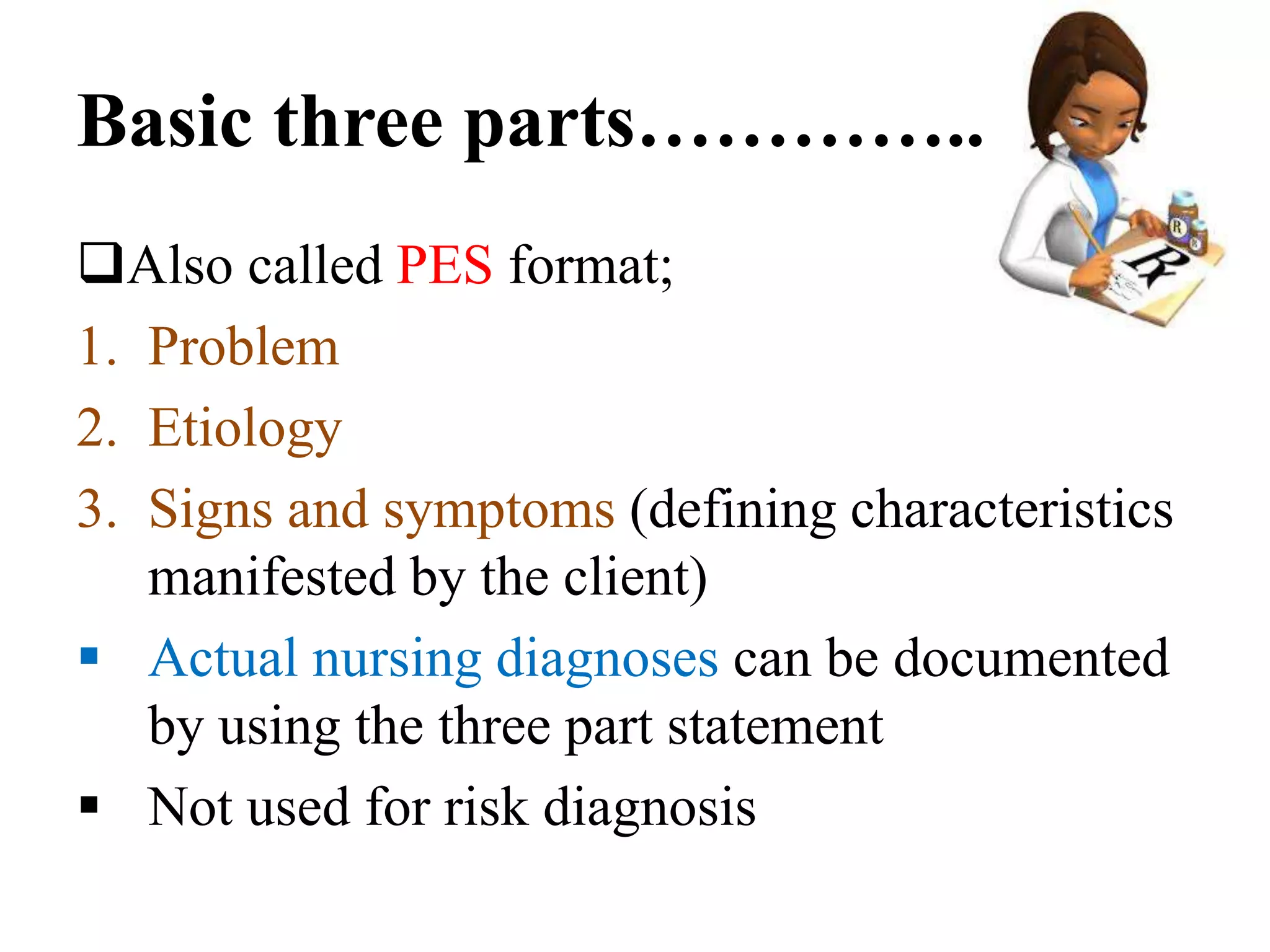









This document discusses the nursing diagnosis process. It begins by introducing nursing diagnosis as the second phase of the nursing process and a pivotal step. It then discusses NANDA's role in developing standardized nursing diagnoses and taxonomy. The document outlines the 13 domains of nursing diagnosis and characteristics such as being clear, evidence-based, and amenable to nursing intervention. It describes different types of diagnoses and provides examples. Finally, it discusses formulating diagnostic statements, including one, two and three part statements, and qualities of accurate diagnostic statements.






































![Nursing_diagnosis[1][1].pptxxxxxxxxxxsjjsk](https://cdn.slidesharecdn.com/ss_thumbnails/nursingdiagnosis11-250803091920-eb89e50b-thumbnail.jpg?width=640&height=640&fit=bounds)
















































