Download as PDF, PPTX
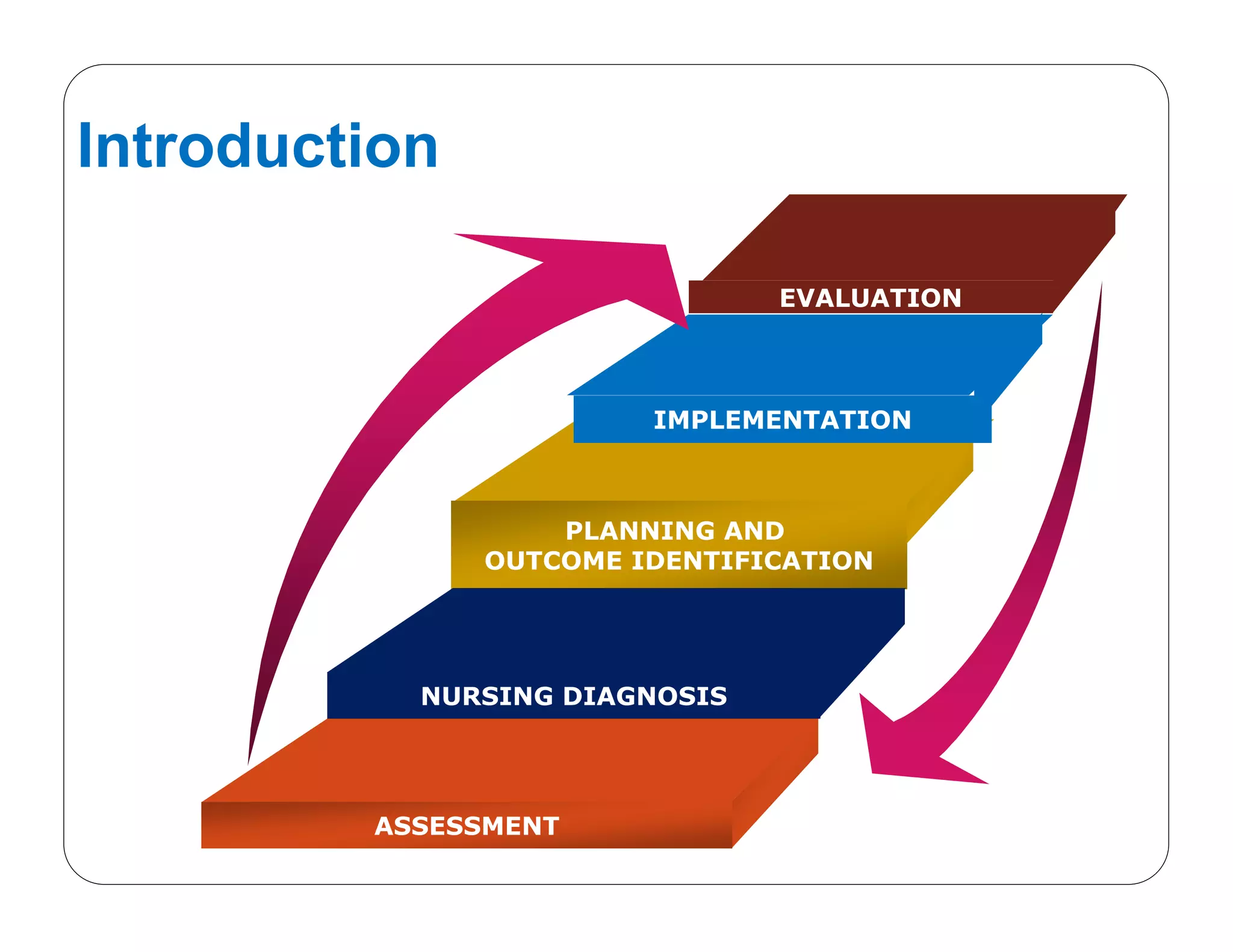
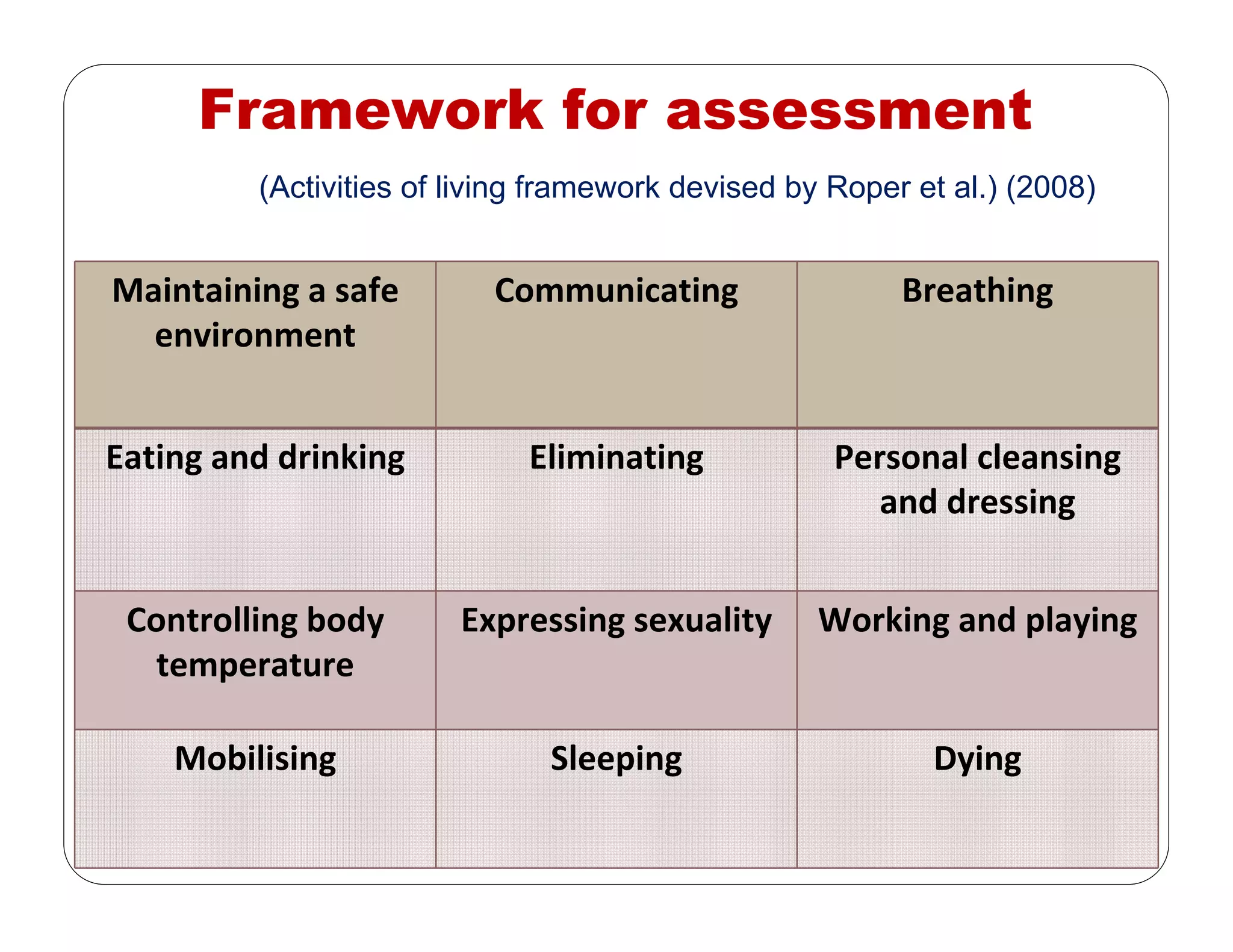

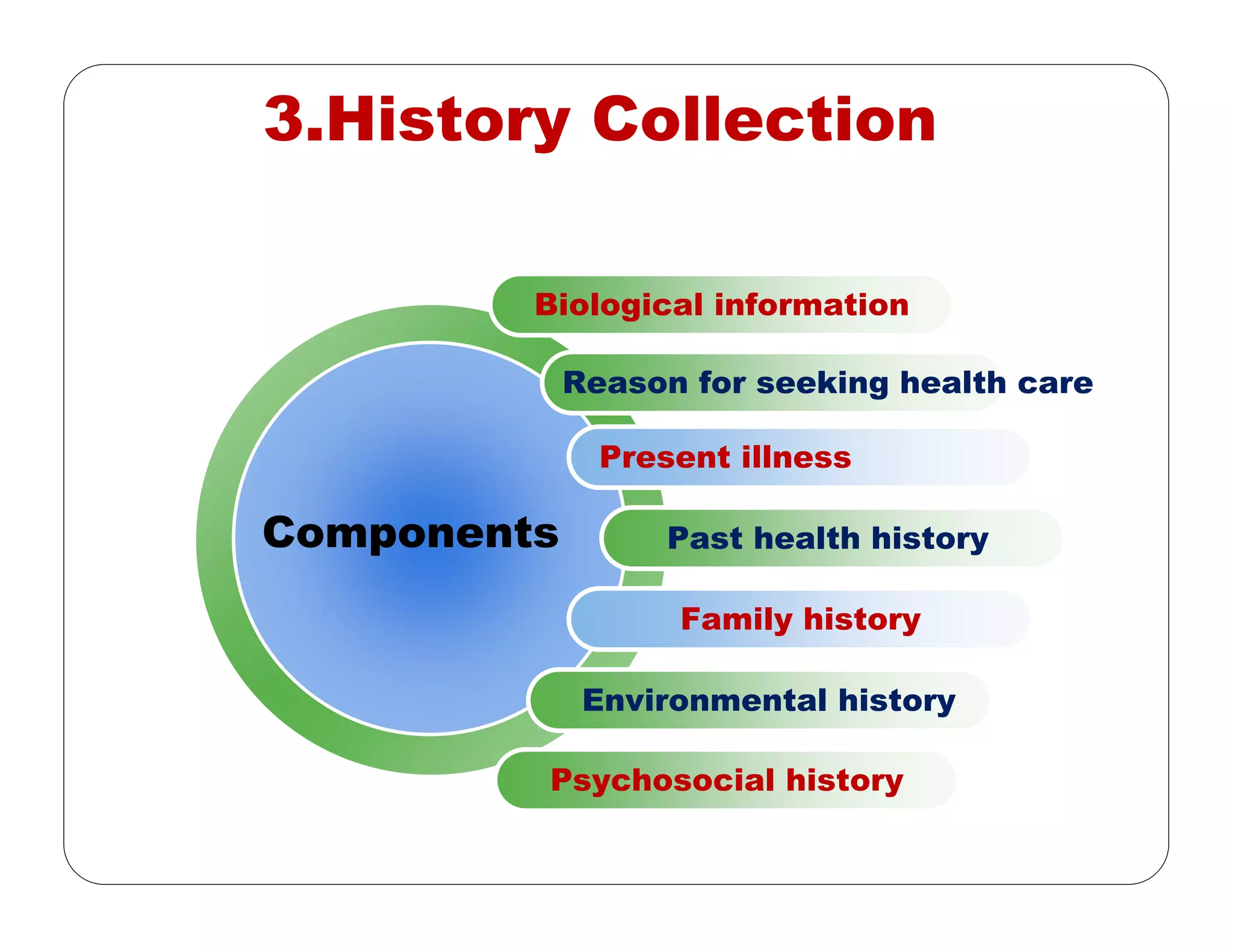
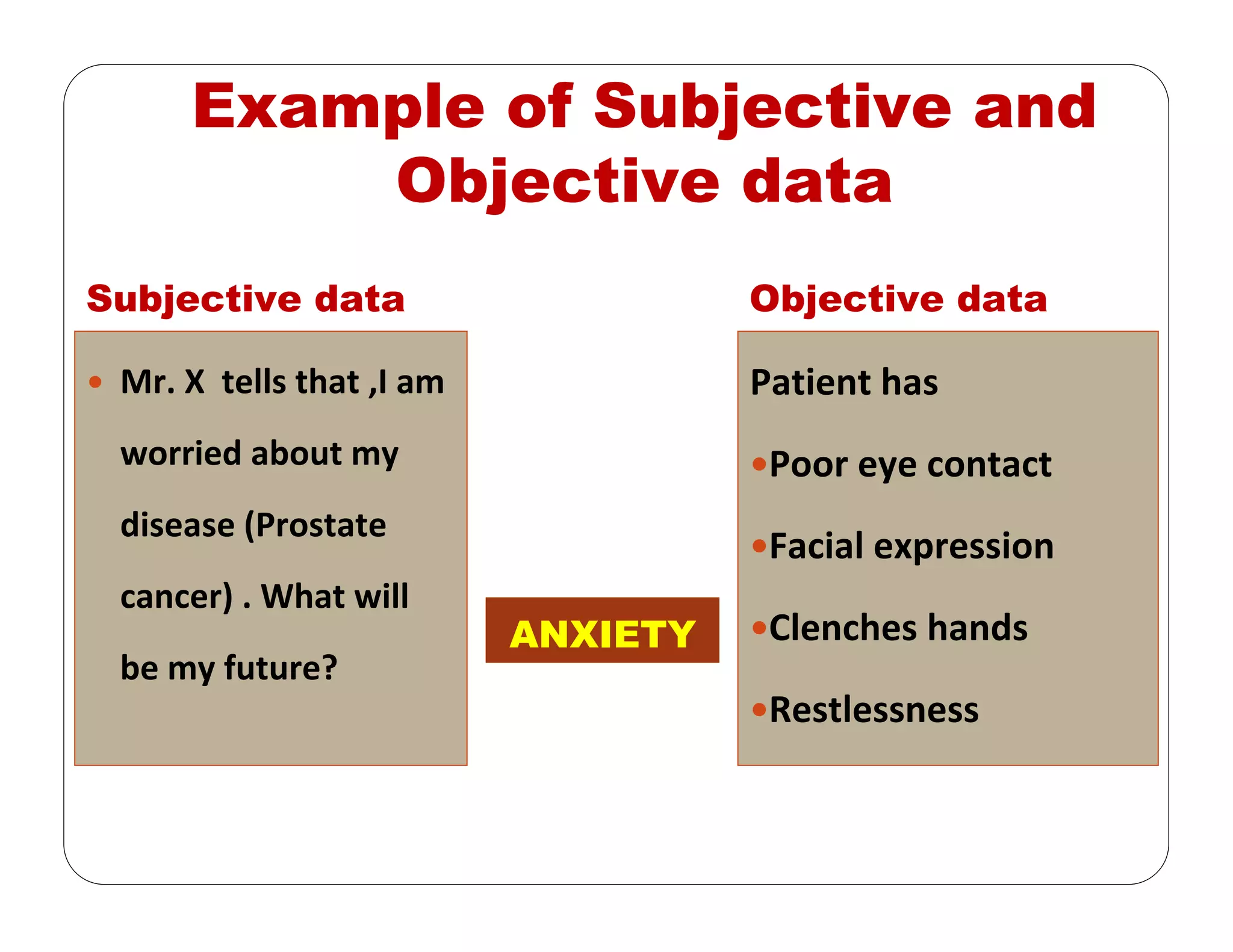
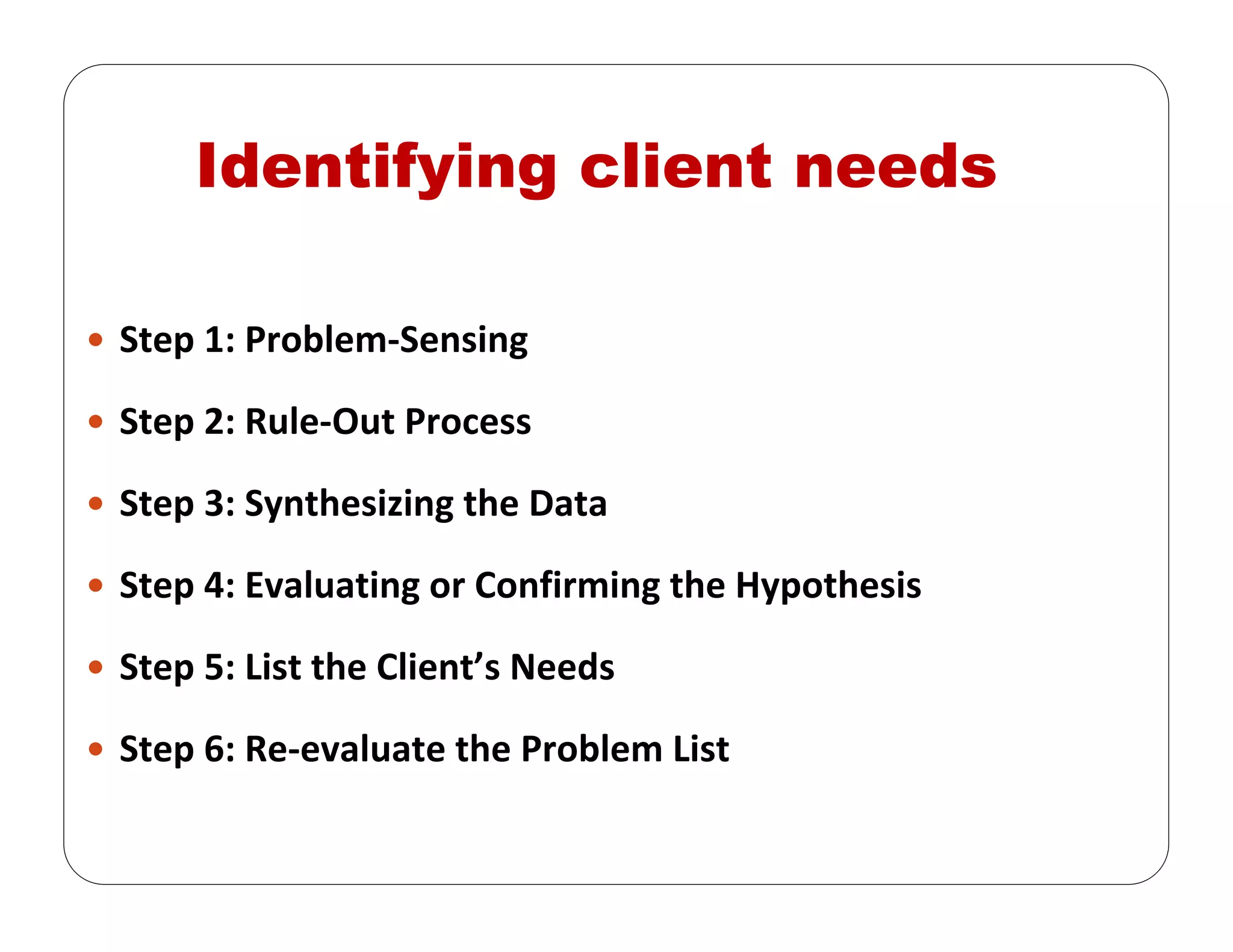
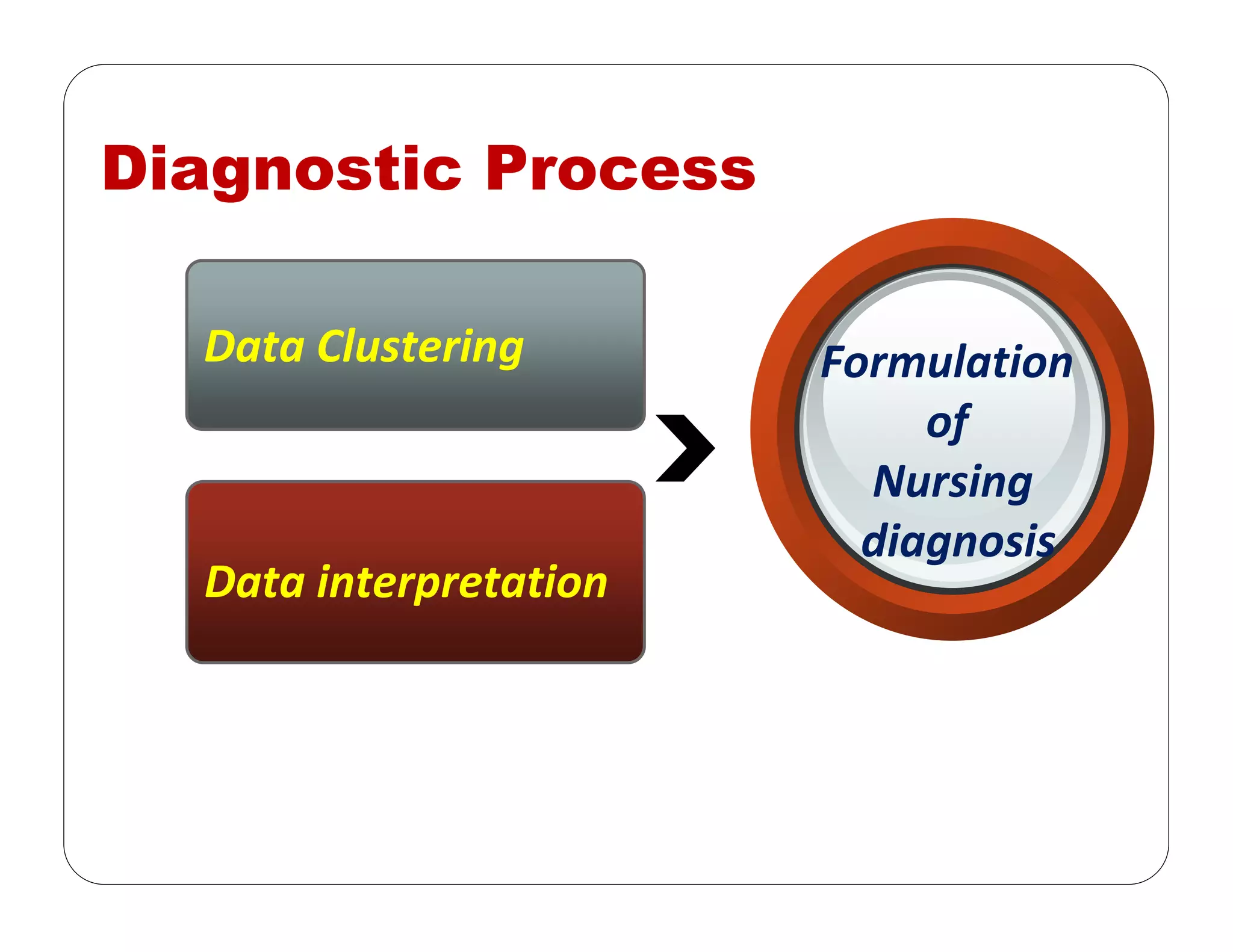

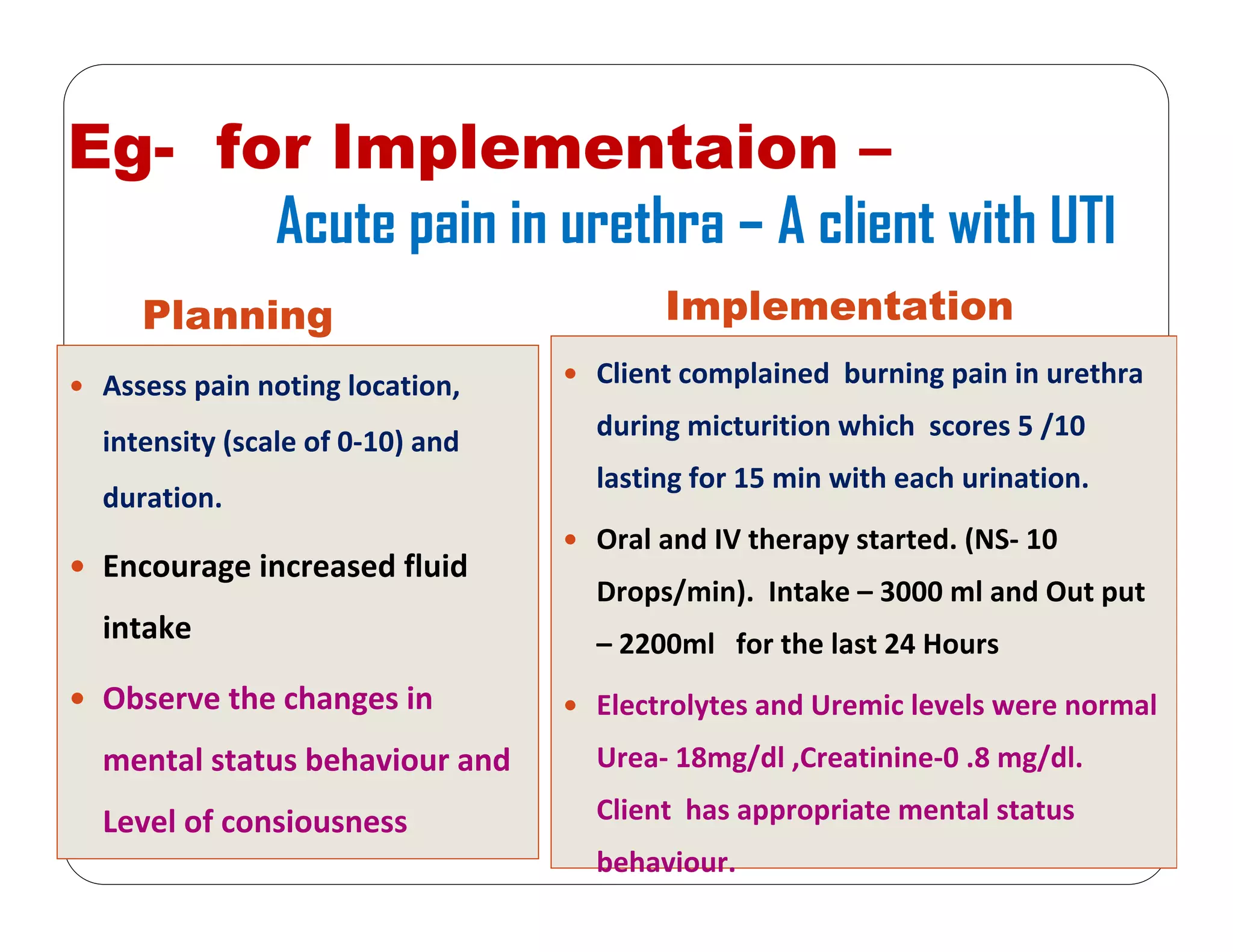
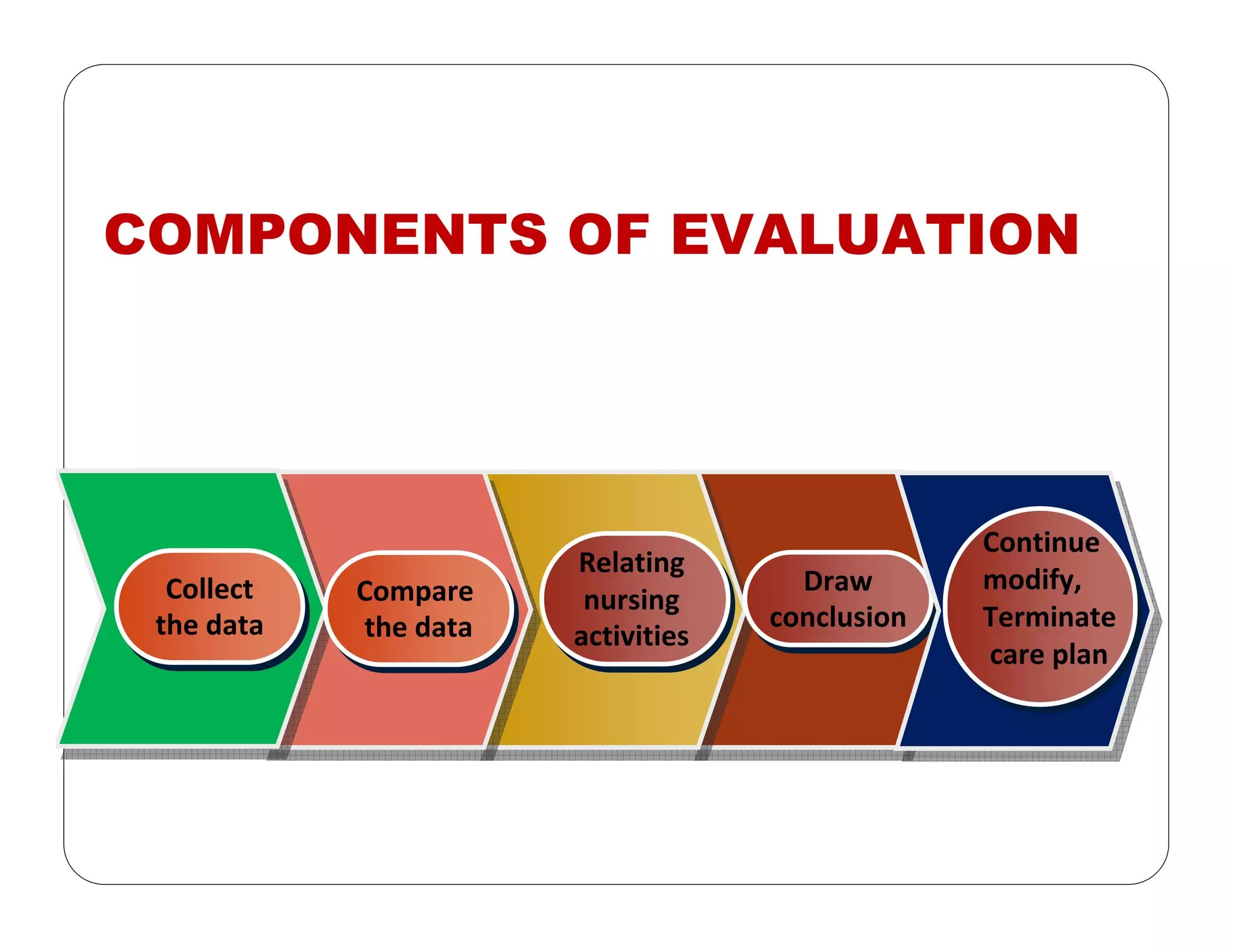


This document outlines the nursing process, emphasizing the importance of assessment, planning, implementation, and evaluation in nursing care. It details various types and methods of nursing assessments, the diagnostic process for identifying patient needs, and the planning and execution of nursing interventions. Additionally, it highlights the significance of documenting and evaluating care to ensure effective patient outcomes.














































![FON 2nd Sam' all slides of 2k23_by_Samiii[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/fon2ndsamallslidesof2k23bysamiii1-240825081529-94f2e683-thumbnail.jpg?width=640&height=640&fit=bounds)






















![Understanding Parkinson’s Disease: Causes, Symptoms, and Treatment [2025]](https://cdn.slidesharecdn.com/ss_thumbnails/understandingparkinson-251208102525-80ba3223-thumbnail.jpg?width=640&height=640&fit=bounds)









