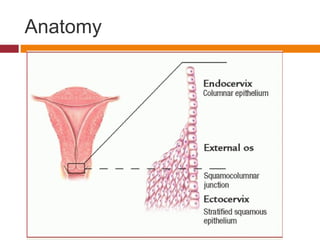
This document summarizes the anatomy, histology, and pathologies of the uterine cervix. It discusses the normal cervix epithelium and how cervical inflammation and infections can cause conditions like cervicitis. Precancerous lesions like cervical intraepithelial neoplasia are often caused by human papillomavirus infection and can progress to invasive cervical cancer if left undetected and untreated. Screening methods like the Pap test aim to detect these early lesions to prevent cervical cancer.

![Normal cervix [gross] - nulliparous woman](https://image.slidesharecdn.com/cervix-170924124127/85/Cervix-4-320.jpg)



![INFLAMMATIONS:
ACUTE & CHRONIC CERVICITIS:
Gonococci,
Chlamydiae,
Mycoplasmas,
Herpes virus [type 2],
Tuberculosis,
[sterility]](https://image.slidesharecdn.com/cervix-170924124127/85/Cervix-8-320.jpg)









![Human Papilloma Virus [HPV]
Vulvar condyloma acuminatum,
Vulvar & vaginal squamous cell
carcinomas,
85% cervical cancers,
90% condylomata & precancerous lesions;
DNA virus](https://image.slidesharecdn.com/cervix-170924124127/85/Cervix-18-320.jpg)



![SQUAMOUS
DIFFERENTIATION
Infection
basal cells
Early (Non-structural)
protein synthesis
LATENTLATENT
INFECTIONINFECTION
Condyloma
or CIN-1
[koilocytosis]
Integration[ISH]
+ Oncogenes
- Tumour suppressor genes
INVASIVE
CARCINOMA
Productive
DNA synthesis
Late [capsid]Late [capsid]
protein synthesisprotein synthesis
[IH][IH]
Viral
particles [EM]
DesquamationDesquamation
transmissiontransmission
HPV life cycle
Episomal DNA
replication (ISH)](https://image.slidesharecdn.com/cervix-170924124127/85/Cervix-22-320.jpg)

















![Chronic cervicitis with moderate dysplasia [ CIN - II ]](https://image.slidesharecdn.com/cervix-170924124127/85/Cervix-40-320.jpg)




































































































