Downloaded 19 times



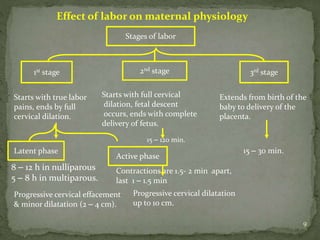
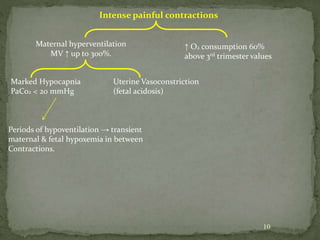
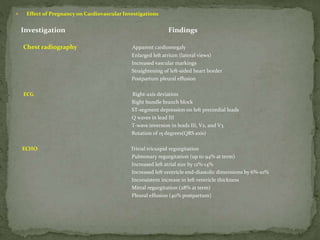
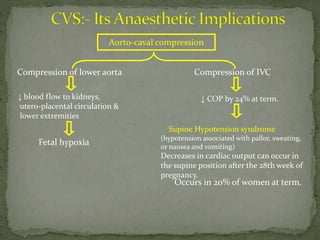
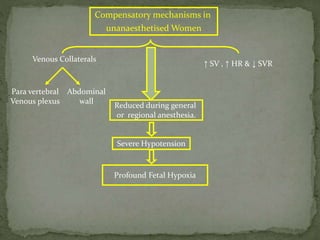
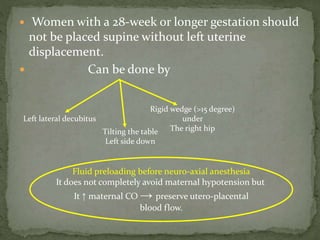



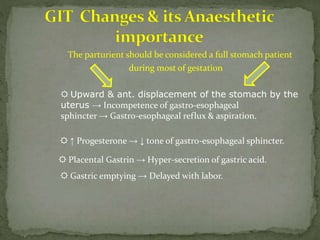

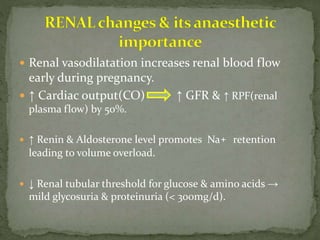
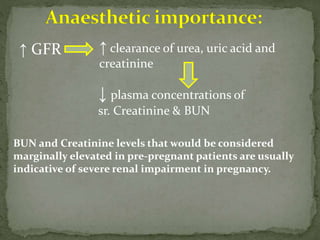
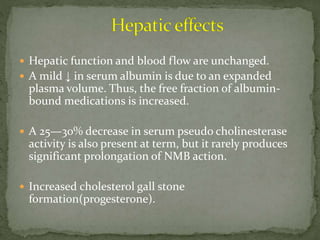
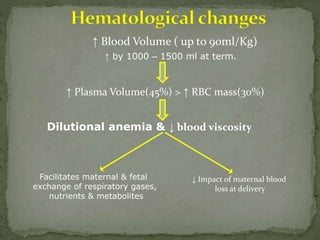

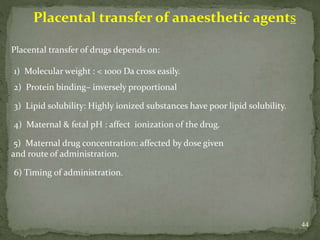

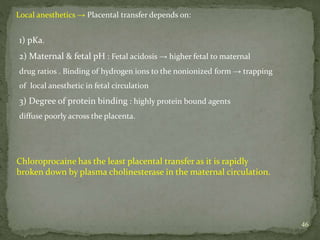
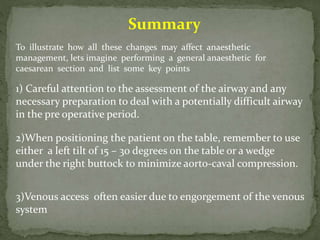
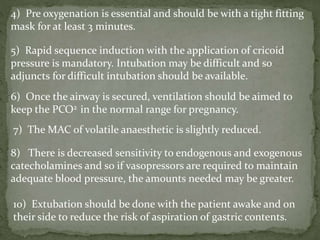


This document summarizes several physiological changes that occur during pregnancy. Key changes include increased blood volume, cardiac output, and respiratory rate. Hormonal changes lead to decreased sensitivity to local anesthetics and inhalational agents. The supine position can cause issues late in pregnancy due to compression of the inferior vena cava and aorta. Regional techniques require lower doses of local anesthetics during pregnancy. Overall, pregnancy results in significant cardiovascular and respiratory adaptations to meet increased metabolic demands of the mother and fetus.




















































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)


