Downloaded 871 times

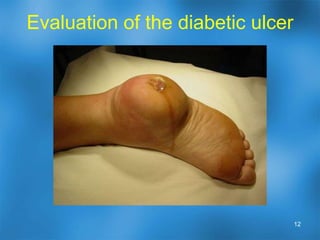

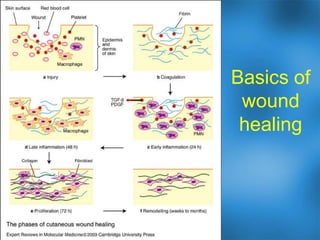



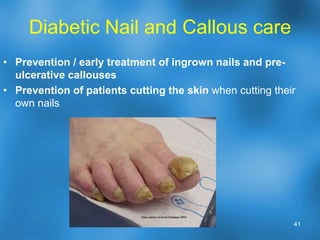
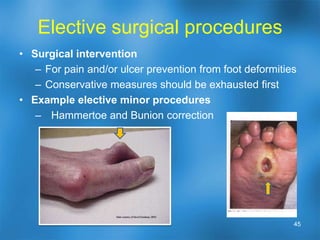


Recent advances in treatments for diabetic foot ulcers have allowed for limbs to be healed that were previously thought unsalvageable, provided a variety of individualized treatment options, and reduced healing times. Key factors that impair wound healing in diabetics include peripheral arterial disease, neuropathy, infection, and structural foot problems. Advanced treatments such as growth factors, skin substitutes, negative pressure therapy, and hyperbaric oxygen can enhance healing when wounds are not responding to traditional care. Recurrent ulcers can be prevented through education, good foot care, appropriate footwear, and surgical correction of deformities when needed.























































































