Dr. Vinay Jain presented on diabetic foot. Some key points:
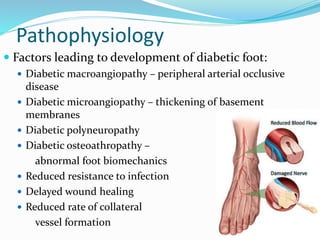
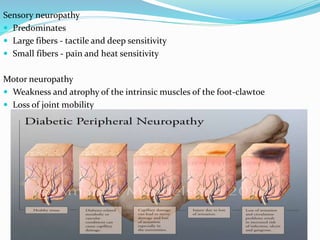
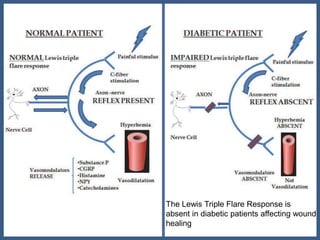
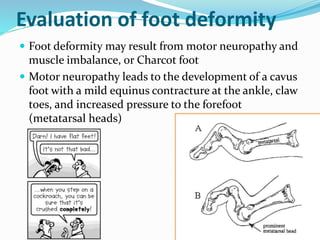
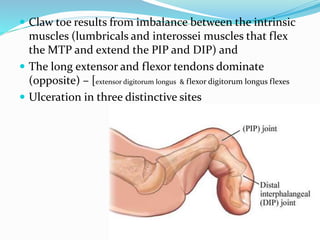
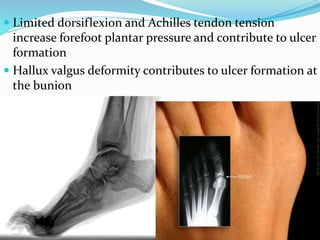
1. Diabetes can cause nerve damage (neuropathy), poor circulation (peripheral arterial disease), and foot deformities which make the feet susceptible to ulcers and infection.
2. About 15% of diabetics develop foot lesions in their lifetime, with an amputation rate 15 times higher than non-diabetics.
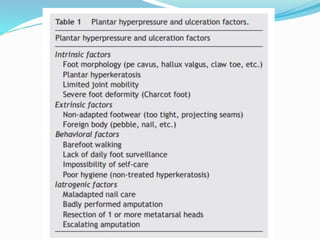
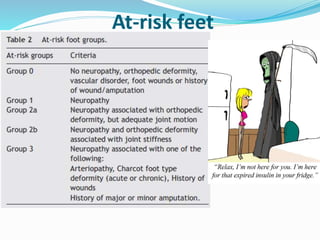
3. Risk factors for foot complications include long diabetes duration, neuropathy, past ulcer/amputation, and poor blood sugar control.
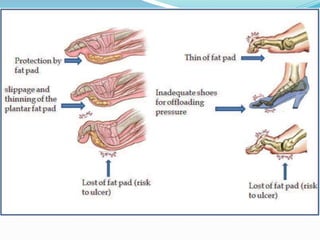
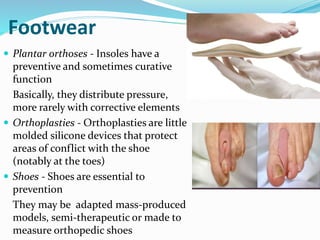
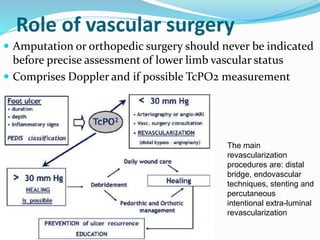
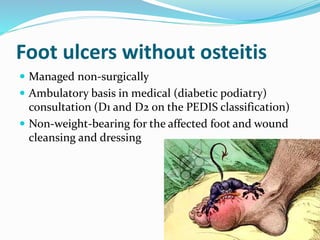
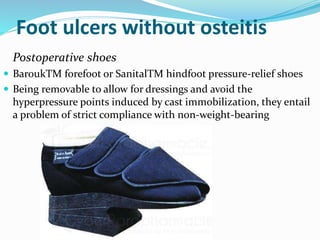
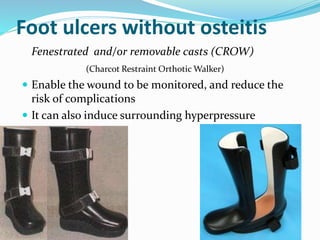
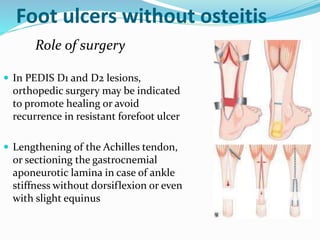
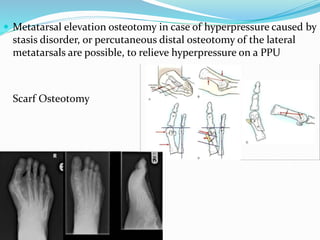
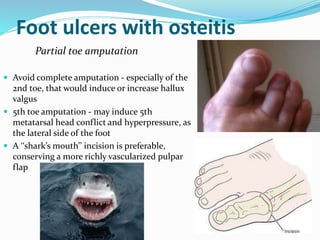
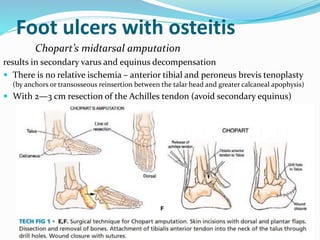
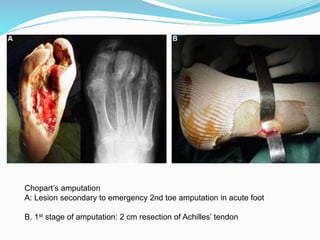
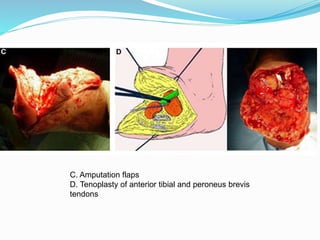
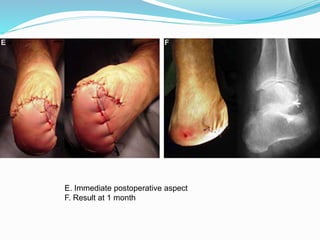
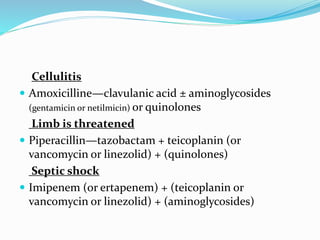
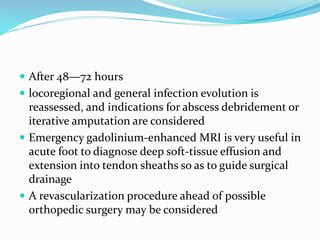
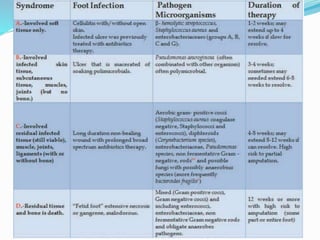
4. Treatment depends on the severity of the ulcer and includes wound cleaning, offloading pressure (casts, special shoes), surgery if needed, and amputation in