Downloaded 121 times





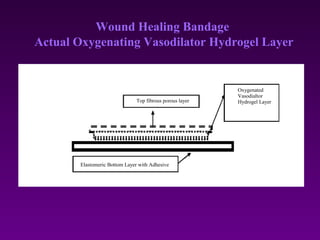
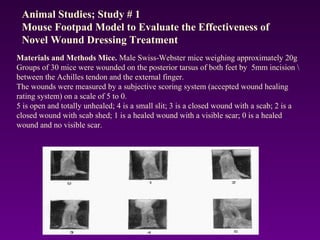

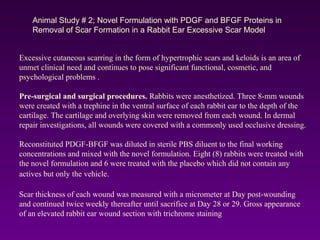



WoundCare Therapeutics Corp is developing novel wound healing technologies based on trans-dermal and trans-mucosal hydrogel aggregates. In animal studies, their oxygenating hydrogel wound dressing was shown to significantly accelerate wound healing compared to regular dressings, reducing wound area by 80% after 7 days versus 29% for controls. A second animal study found their hydrogel formulation containing PDGF and BFGF proteins effectively removed scar formation in a rabbit ear model of excessive scarring. The company aims to license their technologies to partners who can commercialize products for wound healing and dermatology applications.




























































