Downloaded 79 times
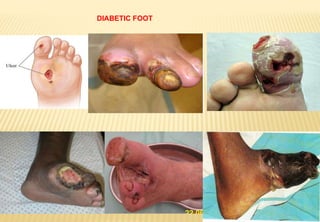
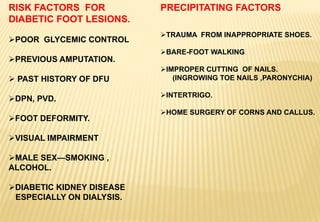
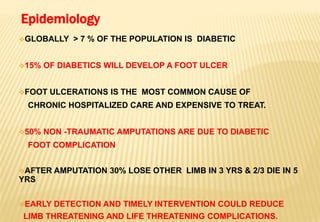
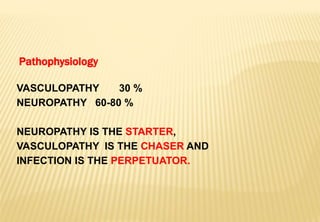
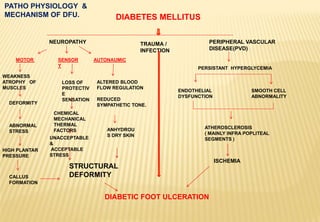
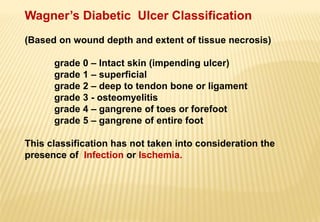
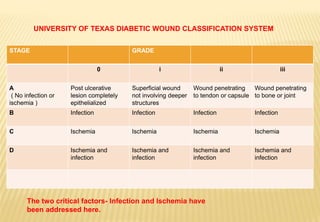



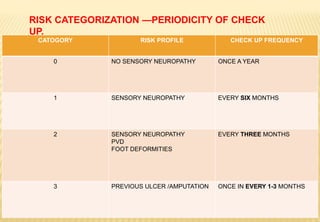
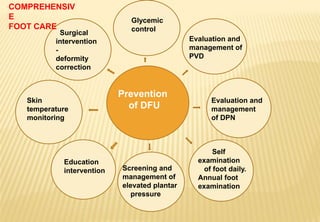

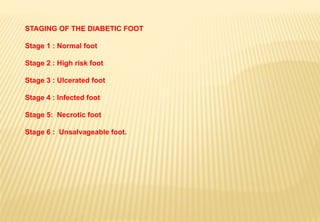

The document provides a comprehensive overview of diabetic foot evaluation and the prevention of diabetic foot ulcers (DFUs), emphasizing the significance of early detection and timely intervention to reduce amputation risk. It outlines various risk factors, classification systems for ulcers, diagnostic assessments, and guidelines for foot care management. The importance of patient education, regular check-ups, and proper footwear is highlighted to prevent complications associated with diabetic foot conditions.



































































