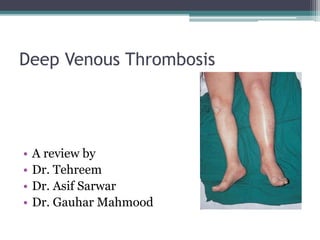
The document discusses deep venous thrombosis (DVT) as a significant cause of pulmonary embolism, emphasizing the importance of early recognition and treatment to reduce morbidity. It outlines various risk factors, anatomical considerations, diagnostic methods, and treatment protocols including anticoagulation and endovascular interventions. The risks of post-thrombotic syndrome are highlighted, along with preventive measures and management strategies.































































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)