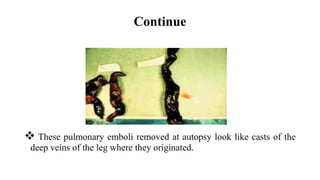
The presentation discusses deep venous thrombosis (DVT), defined as blood clots forming in deep leg veins, with prevalence rates, clinical features, risk factors, and management strategies outlined. Significant risks include prolonged immobilization, cancer, and certain medical conditions, with standard management involving anticoagulation and, in some cases, surgical intervention. The prognosis is critical, as untreated DVT can lead to fatal pulmonary embolism, highlighting the importance of early detection and treatment.


















![Neurophysiological facilitation of respiration [npf]](https://cdn.slidesharecdn.com/ss_thumbnails/neurophysiologicalfacilitationofrespirationnpf-180714163516-thumbnail.jpg?width=640&height=640&fit=bounds)


























































