Download to read offline
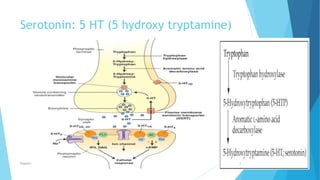
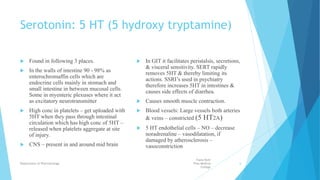




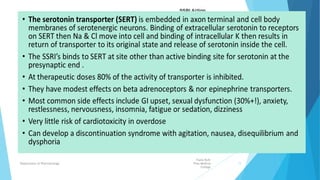

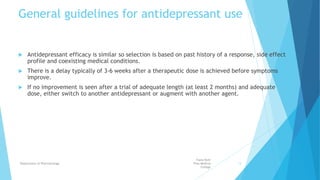







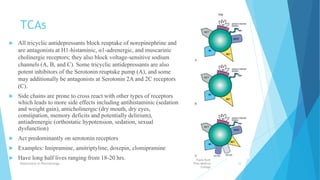


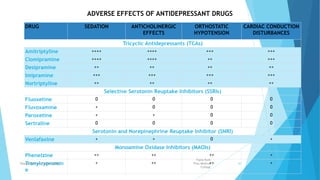


The document discusses the pathogenesis of depression, mechanisms of serotonin synthesis, reuptake, and the classification of various antidepressant drugs including SSRIs, SNRIs, and MAOIs. It details the physiological roles of serotonin in the body, its receptors, and the effects of different antidepressants on serotonin levels. Additionally, it covers general guidelines for antidepressant use, their side effects, and the implications of serotonin modulation in treating anxiety and depression.





























![Down syndrome (2)[1].pptx pediatric lecture](https://cdn.slidesharecdn.com/ss_thumbnails/downsyndrome21-240709094926-fcdd02d9-thumbnail.jpg?width=640&height=640&fit=bounds)










![ABDOMINAL EXAMINATION Presentation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalexaminationpresentation1-240105120242-b6318479-thumbnail.jpg?width=640&height=640&fit=bounds)


























