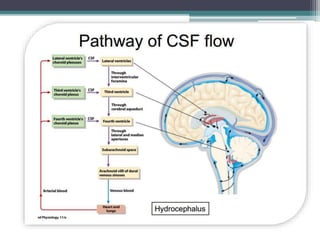
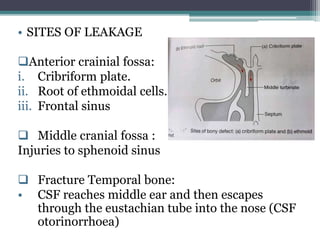
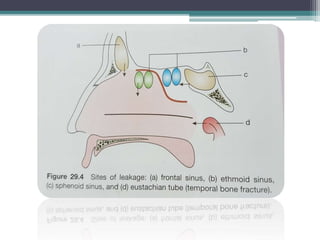
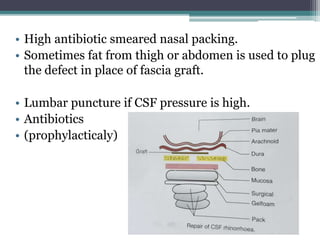
This document discusses cerebrospinal fluid (CSF) rhinorrhea, or the leakage of CSF into the nose. It defines CSF and its circulation and production in the brain. CSF rhinorrhea can be caused by trauma, infections, tumors, or congenital lesions that damage the skull base and allow CSF to leak into the nasal cavity. Diagnosis involves identifying clear fluid leaking from the nose, especially when bending over. Imaging like CT and MRI can localize the leak site. Surgical repair of the skull defect is often needed using grafts and nasal packing.
























































![CSF rhinorrhea in Craniofacial Trauma[Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/csfrhinorrheaautosaved-260206163910-49592e6e-thumbnail.jpg?width=640&height=640&fit=bounds)
![CSF_RHINORHEA[1] ABI.pptx This is imp topic of ENT](https://cdn.slidesharecdn.com/ss_thumbnails/csfrhinorhea1abi-260211113550-42444d5d-thumbnail.jpg?width=640&height=640&fit=bounds)




















