Download to read offline

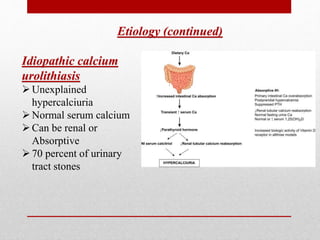


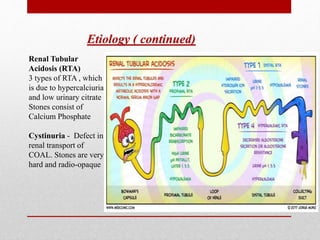





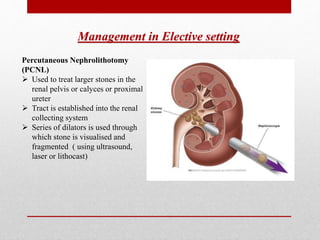


The document discusses renal stone diseases (nephrolithiasis) covering their etiology, symptoms, and management strategies. Types of stones include calcium oxalate, uric acid, and struvite, with conditions like idiopathic calcium urolithiasis and various hypercalcemic disorders listed as causes. Management can be emergency or elective, using interventions such as extracorporeal shockwave lithotripsy, ureteroscopy, and percutaneous nephrolithotomy.





























![Down syndrome (2)[1].pptx pediatric lecture](https://cdn.slidesharecdn.com/ss_thumbnails/downsyndrome21-240709094926-fcdd02d9-thumbnail.jpg?width=640&height=640&fit=bounds)









![ABDOMINAL EXAMINATION Presentation[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/abdominalexaminationpresentation1-240105120242-b6318479-thumbnail.jpg?width=640&height=640&fit=bounds)



























