Downloaded 567 times
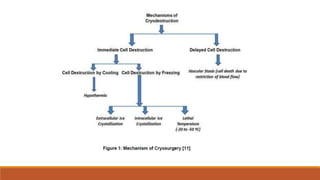
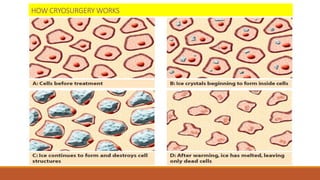
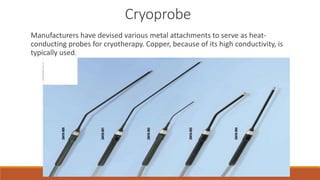


This document provides an overview of cryosurgery. It discusses the history and development of cryosurgery using extreme cold, particularly liquid nitrogen, to destroy diseased tissue. The document outlines the cryosurgery procedure for conditions like prostate cancer, which involves inserting cryoprobes under ultrasound guidance to create ice balls to destroy the tumor. It explains how cryosurgery works through immediate and delayed cell destruction caused by rapid freezing and slow thawing. The document emphasizes the importance of using the lowest possible temperatures, rapid cooling and slow thawing to maximize the effectiveness of cryosurgery.






















































































