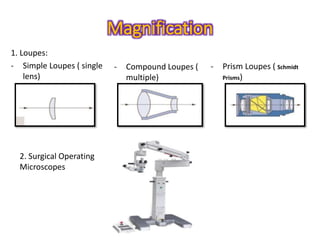
1. Periodontal microsurgery utilizes magnification, improved illumination and specialized instruments to perform periodontal procedures with greater precision and less tissue trauma compared to conventional techniques.
2. The principles of microsurgery include improving fine motor skills, achieving exact wound apposition through passive closure, and use of microinstruments to minimize tissue damage during incision and suturing.
3. Periodontal microsurgery has applications in various periodontal plastic and regenerative procedures and can provide benefits like faster healing and less post-operative discomfort for patients.








































![MIST[1bhjjkkklll do by Jo or ah nu].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mist1-250525215919-08871855-thumbnail.jpg?width=640&height=640&fit=bounds)






































