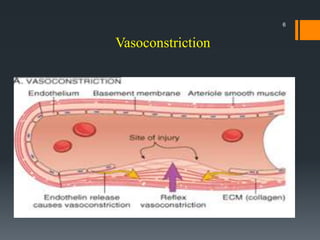
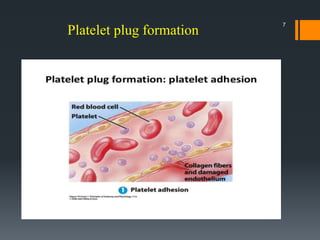
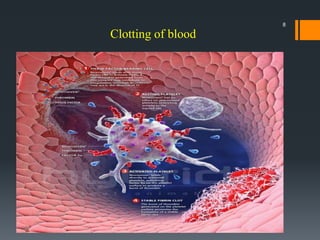
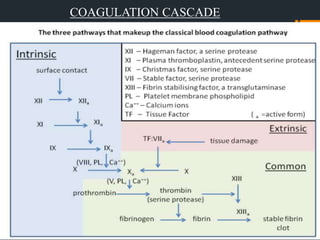
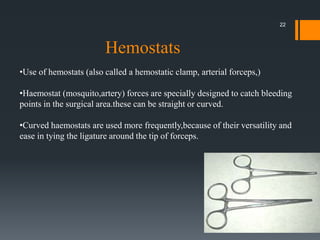
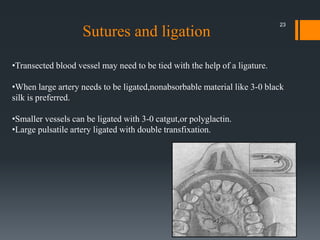
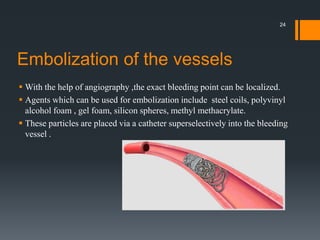
The document discusses management of intraoral bleeding during surgery. It covers hemostasis mechanisms, factors influencing surgical bleeding, adverse effects of bleeding, characteristics of ideal hemostatic agents, and various methods of hemostasis including mechanical, thermal, and chemical approaches. Common hemostatic agents discussed include adrenaline, bone wax, thrombin, gelfoam, and fibrin glue. Proper agent selection and application technique are important to control bleeding during oral surgery procedures.












































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)






![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



