Downloaded 85 times



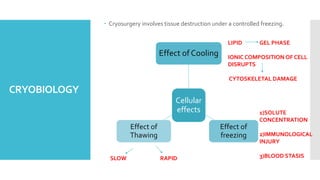






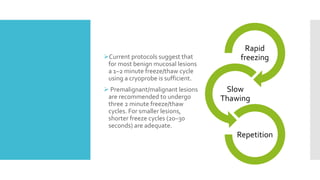



Cryosurgery involves applying low temperatures to living tissues in a controlled manner to induce irreversible damage. It has been used for over 100 years to treat skin lesions. The document discusses the history, indications, contraindications, cryogens, and mechanisms of cryosurgery. It describes open systems using liquid nitrogen spray and closed systems using cryoprobes. Cryosurgery can treat premalignant and benign oral lesions using 1-2 minute freeze/thaw cycles and is an effective minimally invasive treatment option in oral and maxillofacial surgery.




























































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)















