Downloaded 72 times



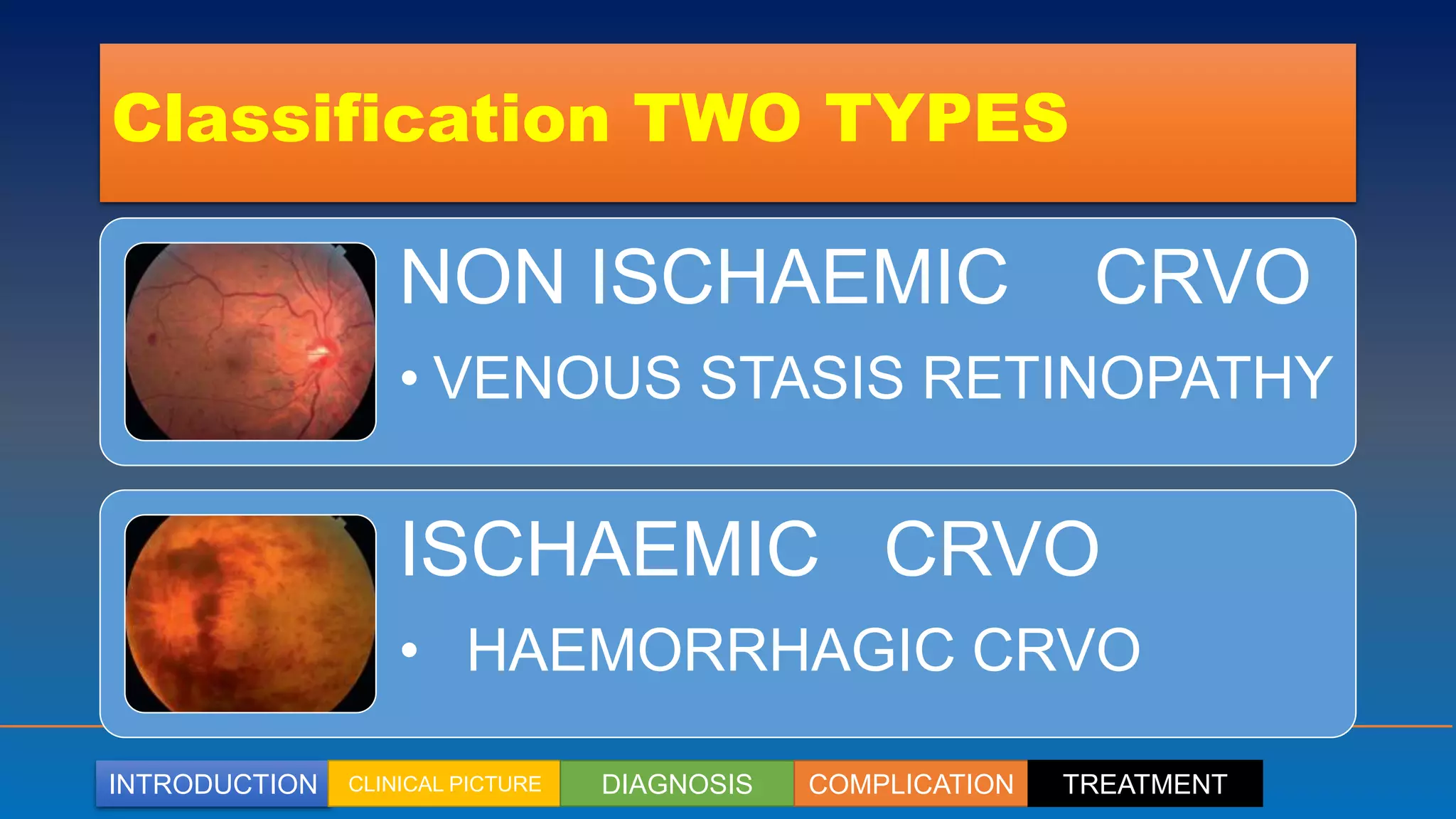























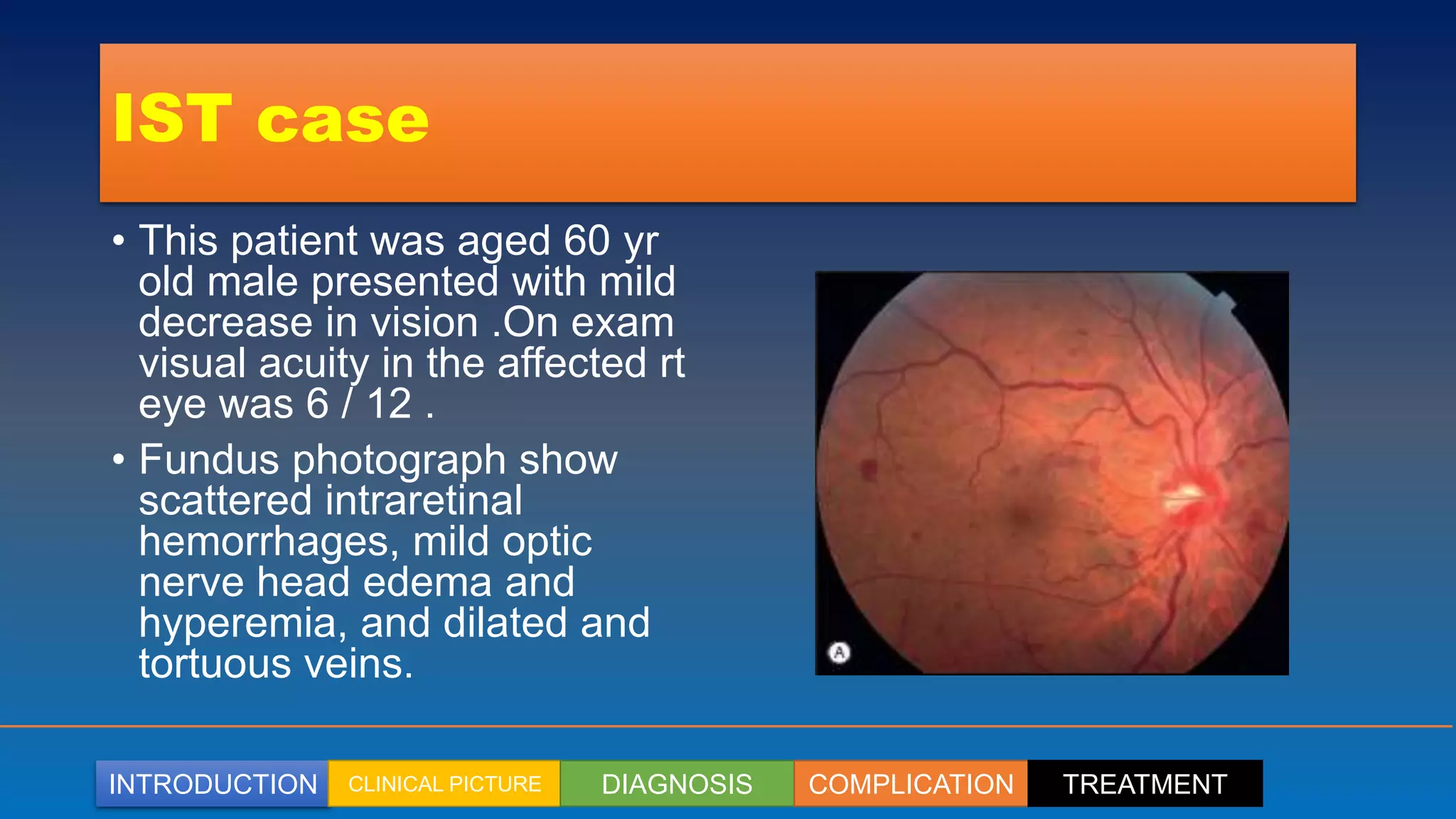
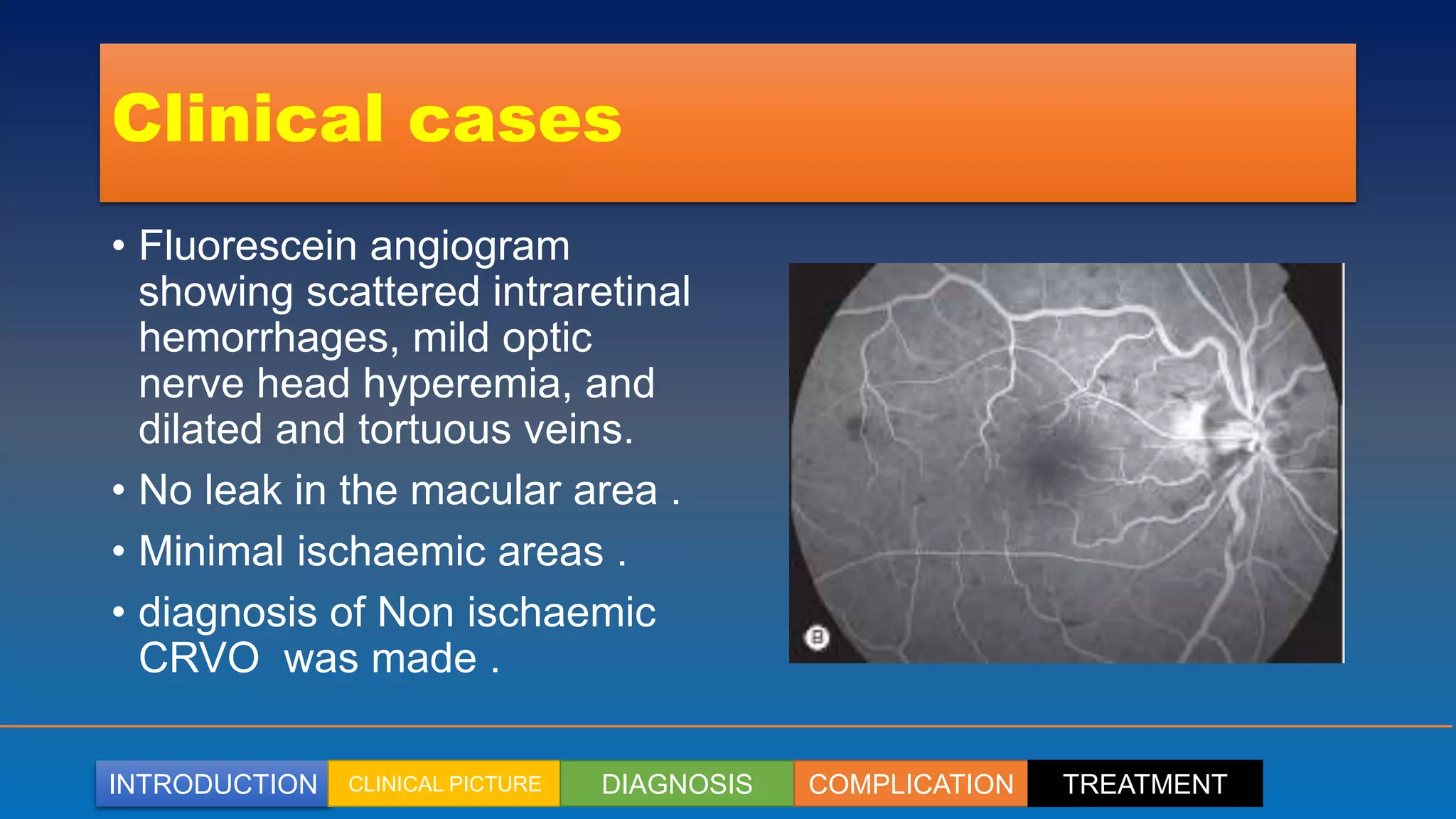
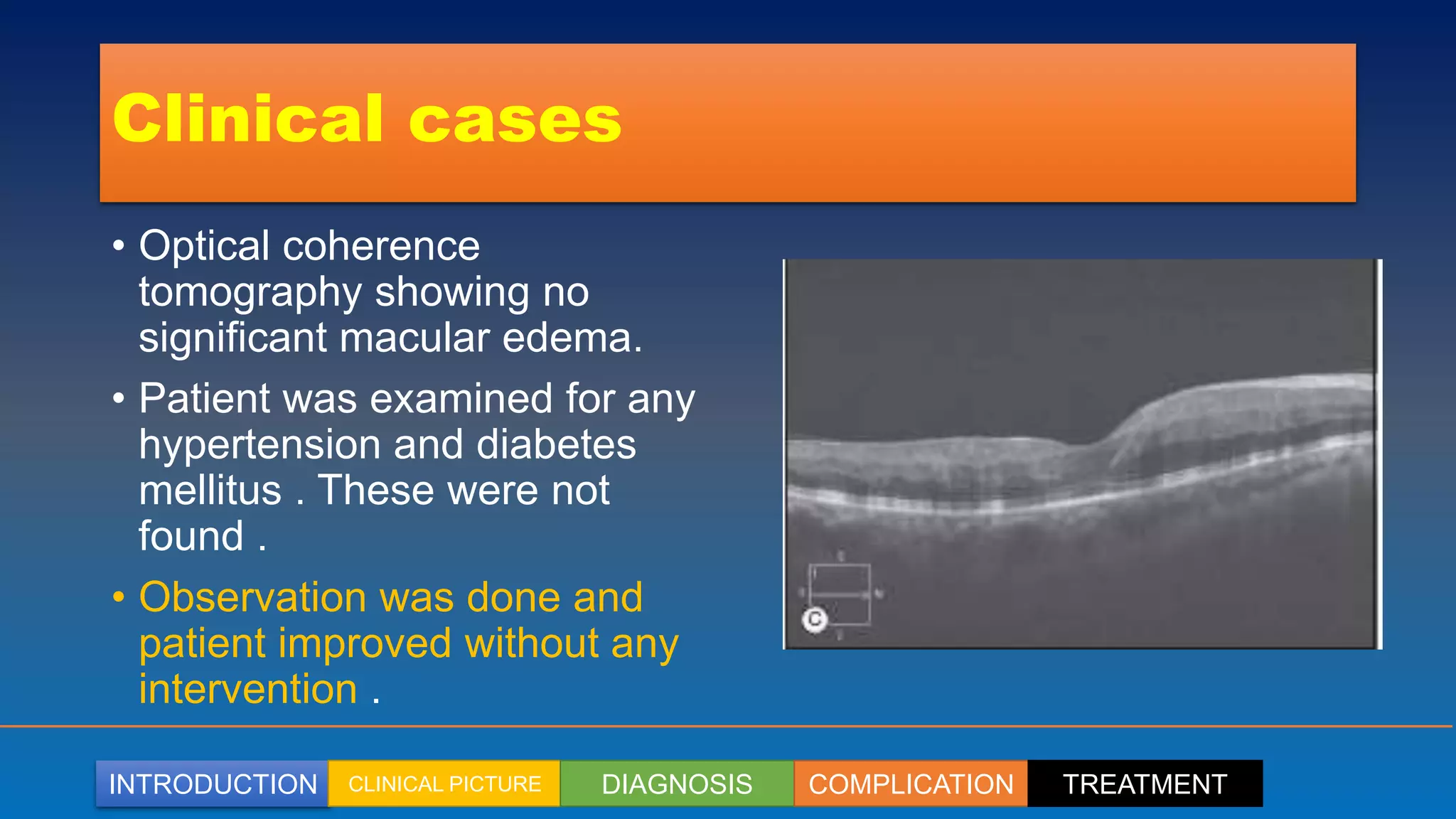







Central retinal vein occlusion (CRVO) primarily affects patients over 60 years and results from venous occlusion due to arteriosclerosis or degeneration, leading to various complications like vision loss and neovascularization. Management includes careful diagnosis, monitoring, and treatment options such as systemic therapy for underlying conditions, intravitreal anti-VEGF agents, and laser therapies, particularly for cases with significant macular edema or neovascularization. Intravitreal pharmacotherapy has become the standard of care for CRVO-associated macular edema, with agents like ranibizumab and dexamethasone showing significant improvement in visual acuity.























































































