Downloaded 47 times



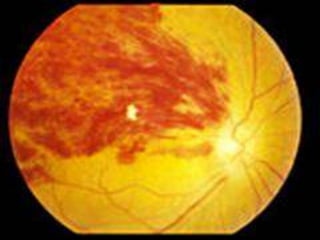


This document discusses central retinal vein occlusion (CRVO), a blockage of the main vein draining the retina. It outlines the etiology (causes like hypertension, diabetes, hyperviscosity), clinical features (sudden vision loss, hemorrhages, edema), investigations (blood tests, imaging), complications (cystoid macular edema, neovascular glaucoma), prognosis, and treatments (anti-VEGF drugs, steroids, laser photocoagulation). It also briefly discusses branch retinal vein occlusion which involves blockage of a retinal branch vein.



































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


















