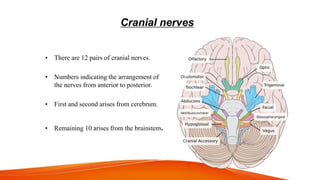
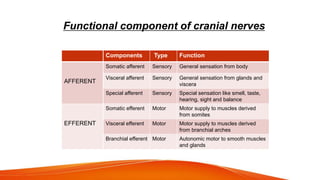
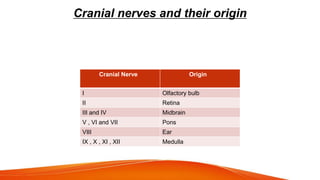
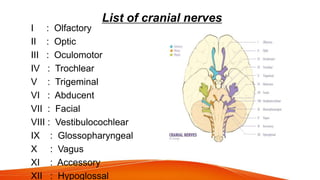
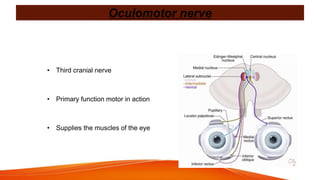
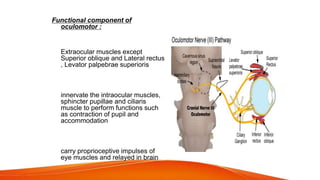
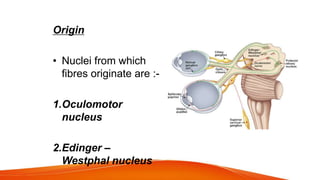
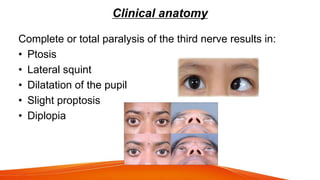
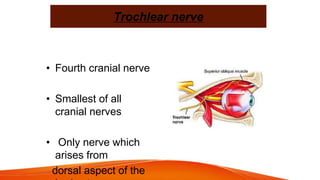
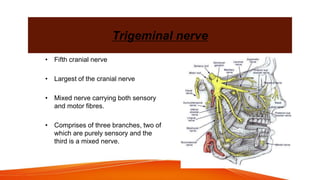
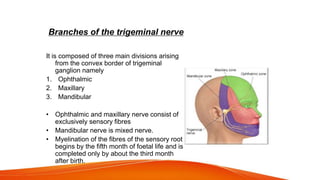
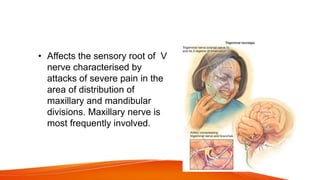
This document provides an overview of the 12 cranial nerves, including their origin, functional components, and branches. It describes each nerve individually, noting their motor, sensory, or mixed functions. For example, it states the oculomotor nerve is mainly motor and supplies the extraocular muscles, while the trigeminal nerve is mixed and provides sensation to the face as well as motor function to muscles of mastication. The document aims to comprehensively describe the cranial nerves, their pathways and roles in a detailed yet organized manner.