Downloaded 13 times


![Monoclonal anribobies for diagnosis of lymphoid disorders
Panel of monoclonal antibodies for the diagnosis of lymphoid
disorders
B cellT cell
First-line SmIg (kappa/lambda), CD19, CD23, FMC7,
mCD79b, mCD22, CD5[*] + CD 20CD2, CD5
Second-line CD11c, CD25, CD103, CD123, CD38, CD138,
CyIgCD3, CD4, CD7, CD8
Optional markers: CD25, CD79a, and natural killer associated (e.g.,
CD16, CD56, CD57, and CD11b).
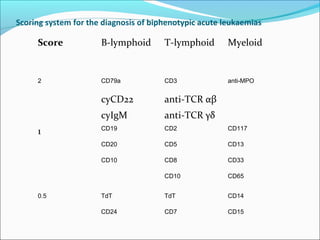
Panel of monoclonal antibodies for the diagnosis of acute
leukaemias
ALLAML B-lineageT-lineage
First-line CD19, CD22, CD79a, CD10[*]CD7, CD2,
cyCD3CD13, CD33, CD117, anti-MPO TdT, HLA-Dr, CD34
Second-linecymu, SmIgCD1a, CD5, CD4, CD8, anti-
TCRCD41, CD42, CD61, anti-glycophorin A
(Optional markers: CD14, antilysozyme, CD36).](https://image.slidesharecdn.com/nhlwithaihadrnazim-150101120026-conversion-gate01/85/Nhl-with-aiha-dr-nazim-55-320.jpg)

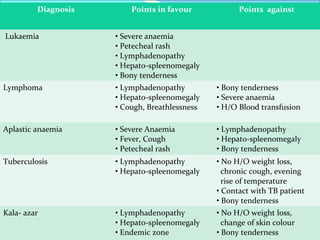
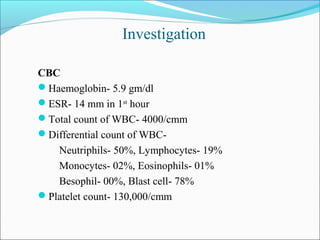
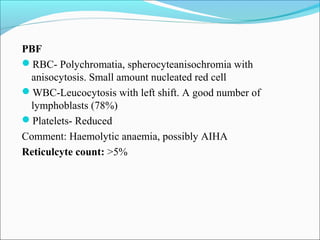
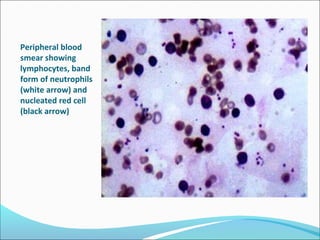
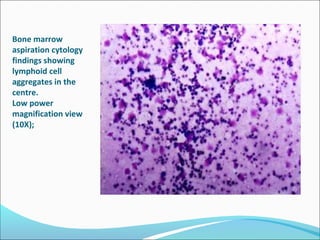
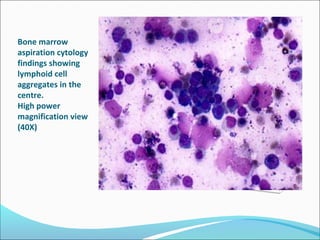
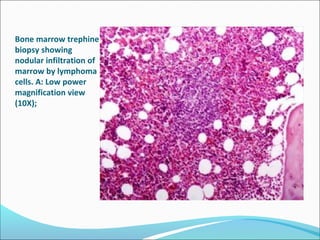
This document presents a case report of a 35-year-old man who presented with fever, night sweats, cough, pallor, fatigue, sore throat, anorexia, lymphadenopathy, hepatosplenomegaly, and bone tenderness over 4 months. Initial biopsy suggested Hodgkin's lymphoma but review suggested non-Hodgkin's lymphoma. Further workup found pancytopenia, lymphoblasts on peripheral smear, and nodular lymphoma infiltration on bone marrow biopsy, consistent with a diagnosis of both NHL and autoimmune hemolytic anemia. The diagnostic challenges and treatment considerations for NHL and its association with autoimmune diseases like AIHA are discussed.

















































































