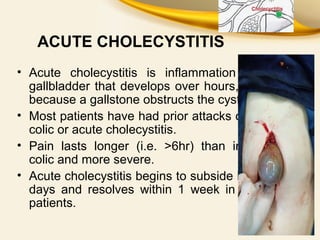
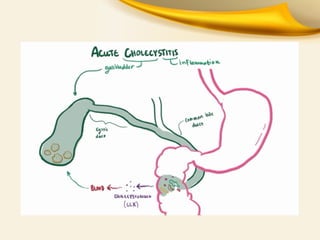
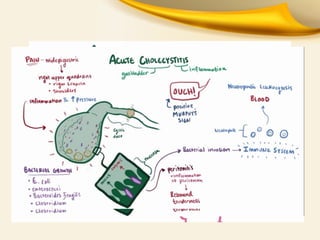
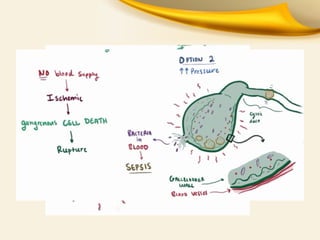
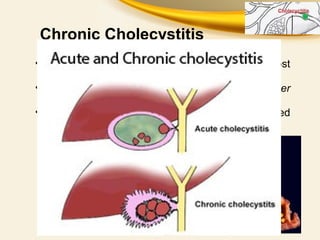
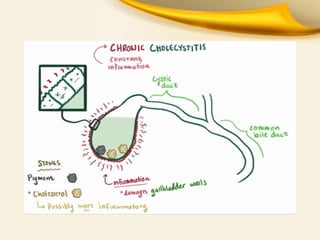
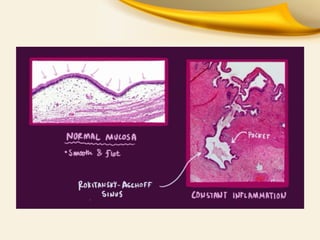
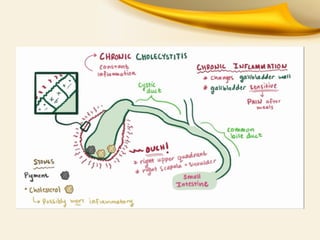
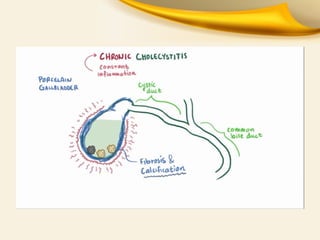
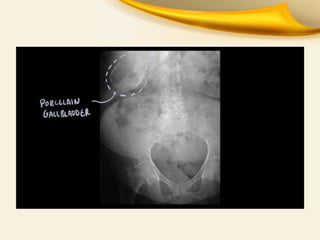
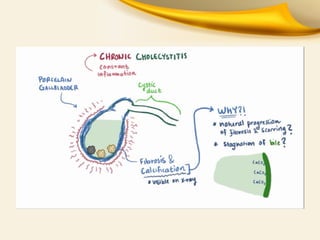
The document discusses acute and chronic cholecystitis, highlighting that acute cholecystitis is primarily caused by gallstone obstruction and characterized by severe, prolonged pain. The diagnosis involves clinical findings, imaging studies, and laboratory tests, with urgent treatment options including cholecystectomy and cholecystostomy for complications. Chronic cholecystitis is often due to gallstones and requires cholecystectomy as well, especially in cases with complications like CBD stones and pancreatitis.