Downloaded 484 times
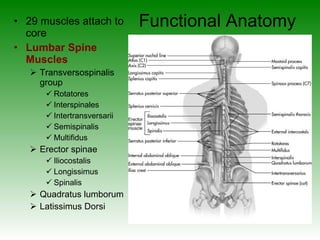

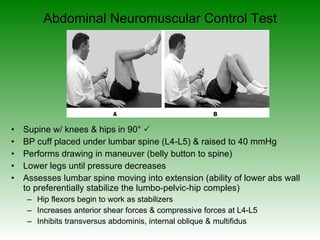

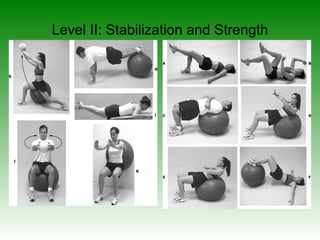
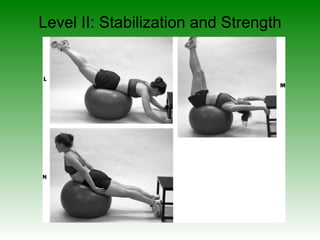
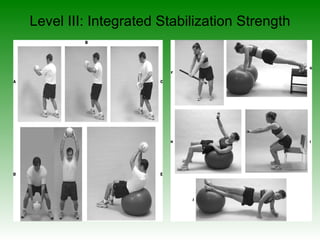
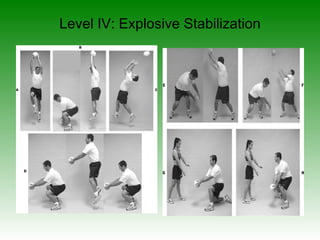

The document discusses the core and its importance for optimal functioning of the kinetic chain. It defines the core as the lumbo-pelvic-hip complex and describes the muscles involved. Various assessment tests are provided to evaluate core strength, endurance, neuromuscular control and overall functionality. Guidelines are given for developing a comprehensive core stabilization training program with emphasis on progression from stabilization to integrated strength training across multiple planes and functional activities.


















































![Prac 9 Therapeutic Ex [Lower].pdfdnxjzjsj](https://cdn.slidesharecdn.com/ss_thumbnails/prac9therapeuticexlower-251217074550-6c2c6de8-thumbnail.jpg?width=640&height=640&fit=bounds)