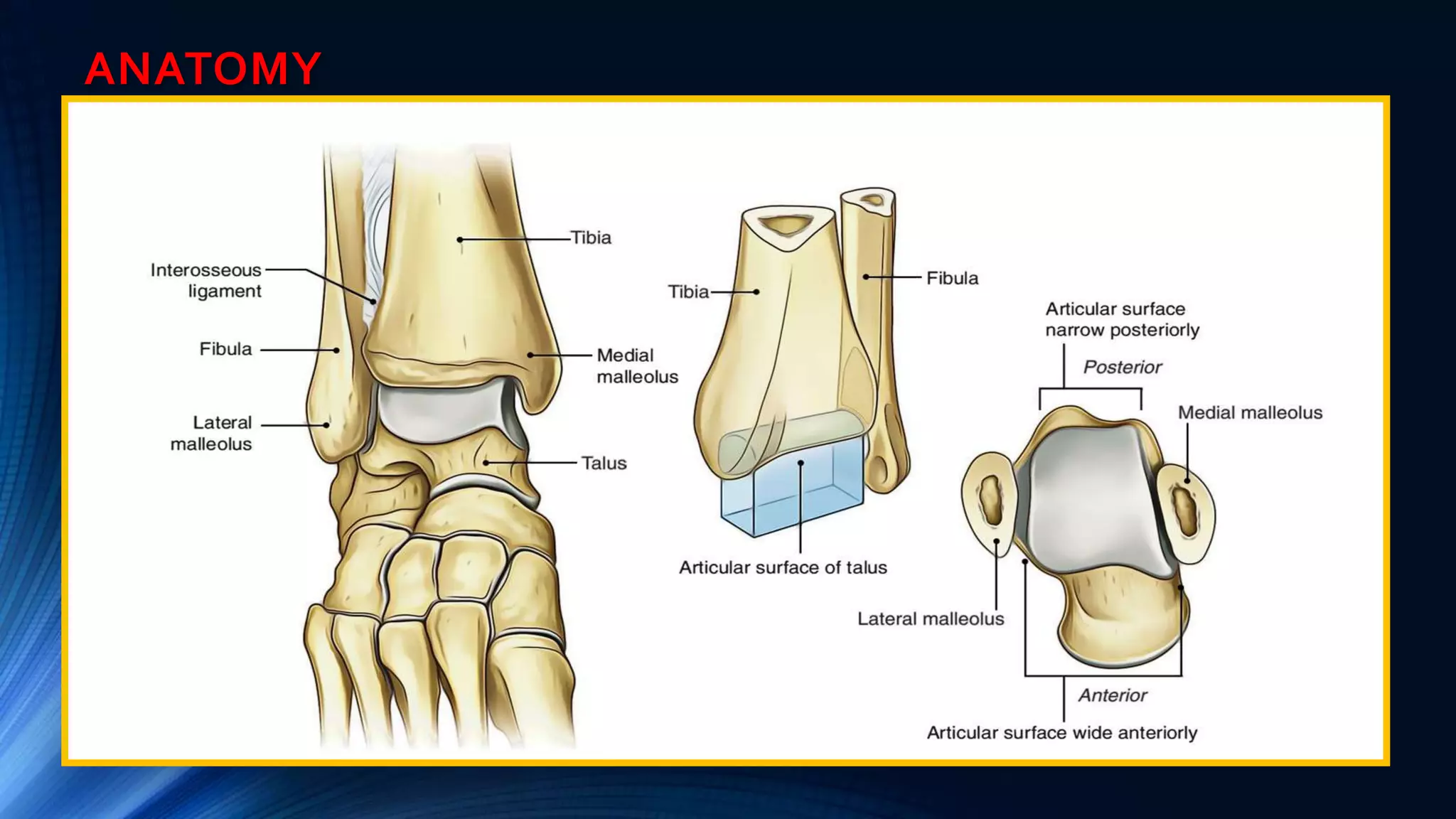
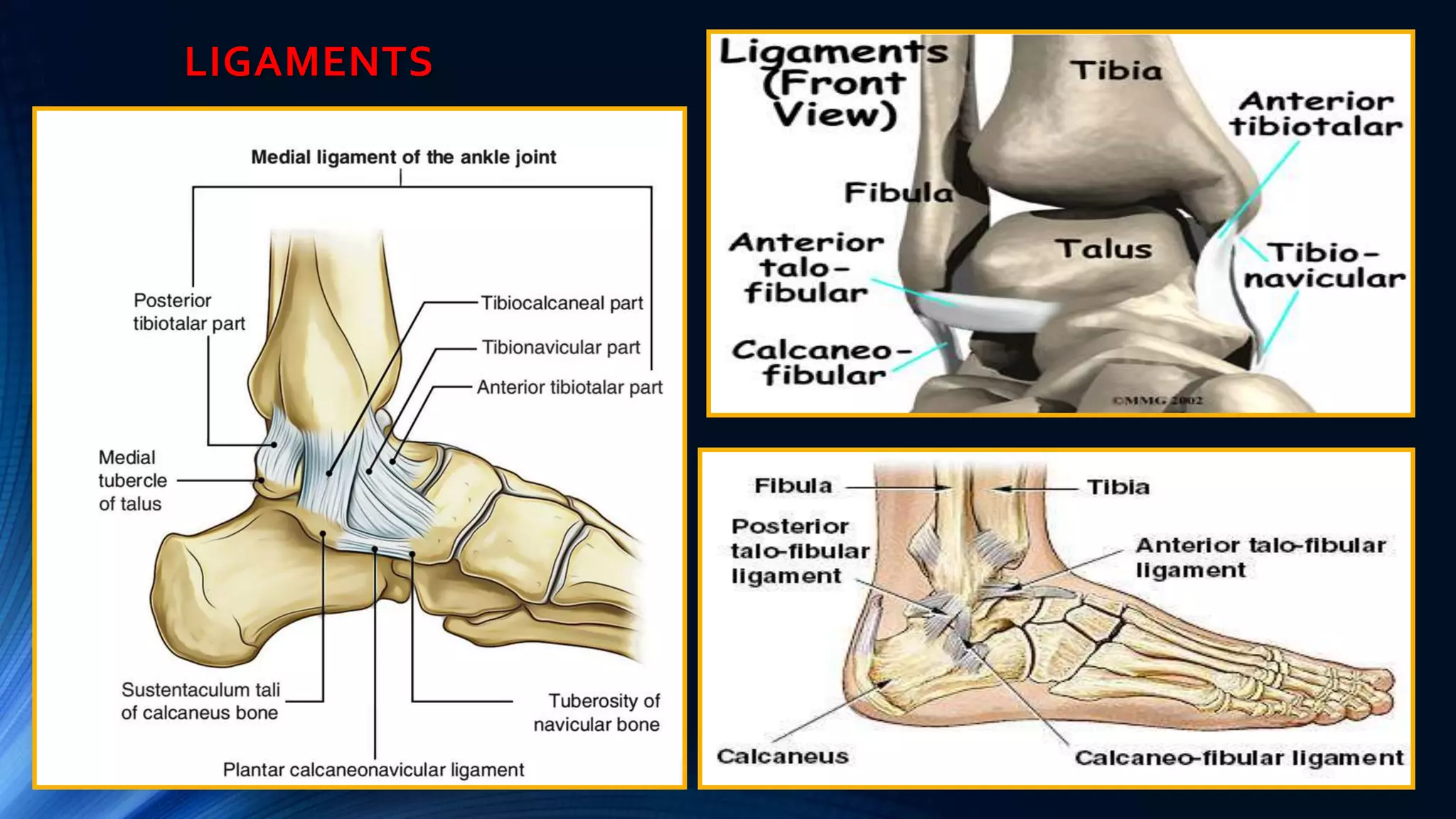
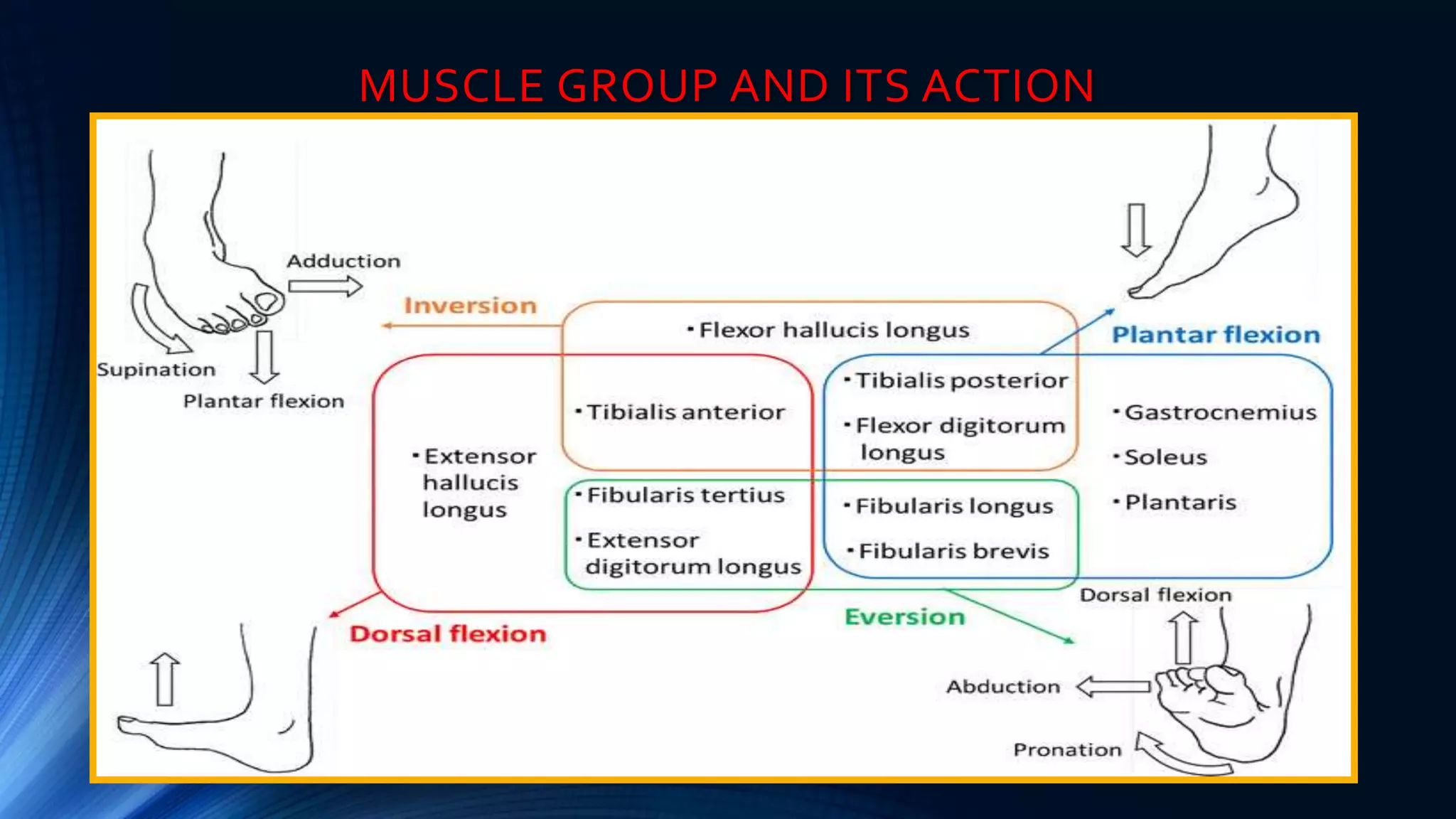
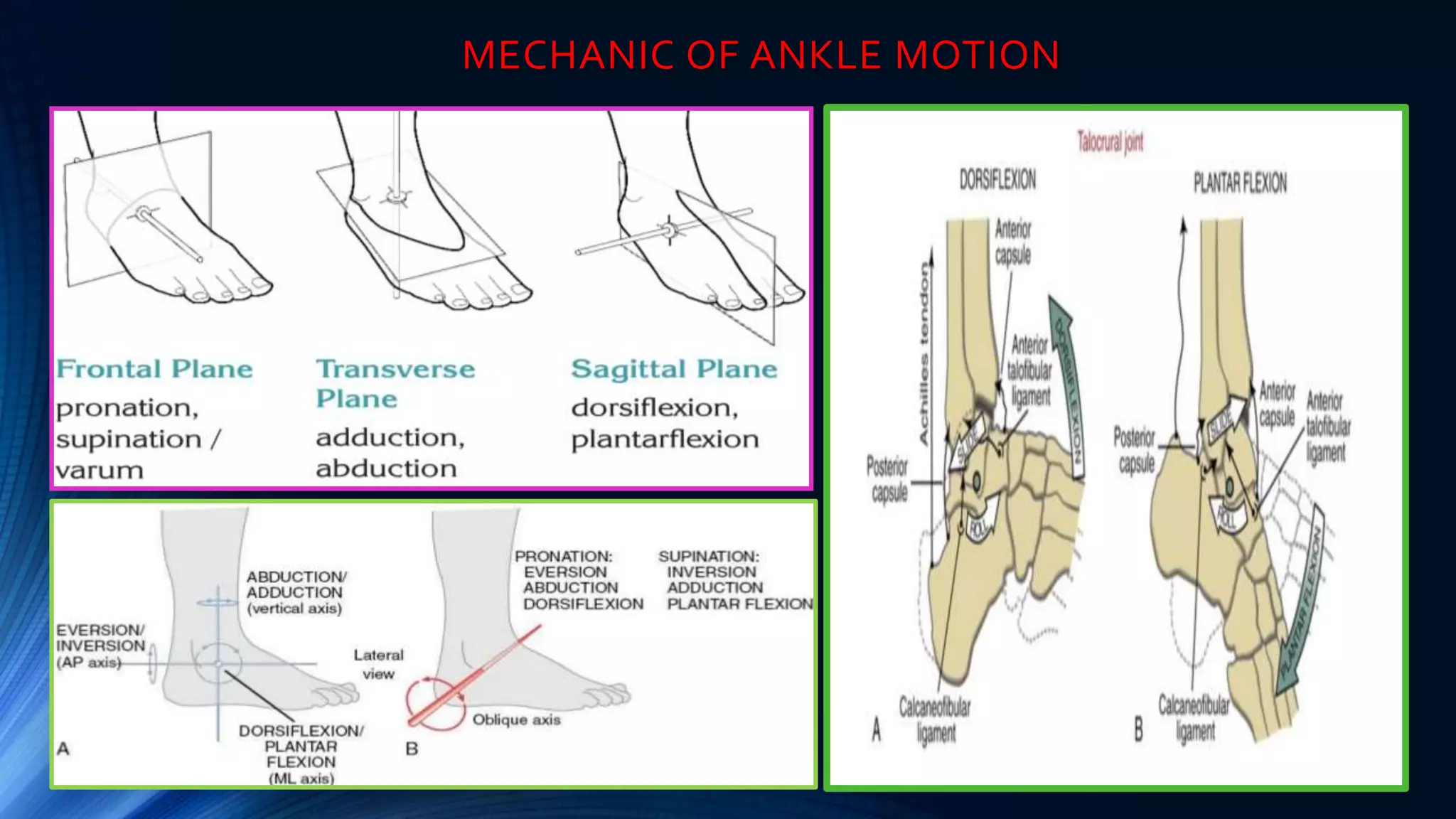
This document discusses the pathomechanics of ankle joint injuries. It begins with the anatomy and ligaments of the ankle joint. It then discusses the muscle groups around the ankle joint and their actions. Next, it explores the mechanics of ankle motion and different types of ankle injuries including lateral and medial ligament injuries, fractures, and muscular imbalances. It provides details on specific muscles like the tibialis anterior and their weaknesses or tightnesses. It concludes with discussing chronic ankle instability and recent literature on lateral ankle sprains and reinjury rates. In summary, the document provides an in-depth overview of ankle joint anatomy, mechanics, common injuries and their pathomechanics, as well as muscular factors.