Downloaded 52 times
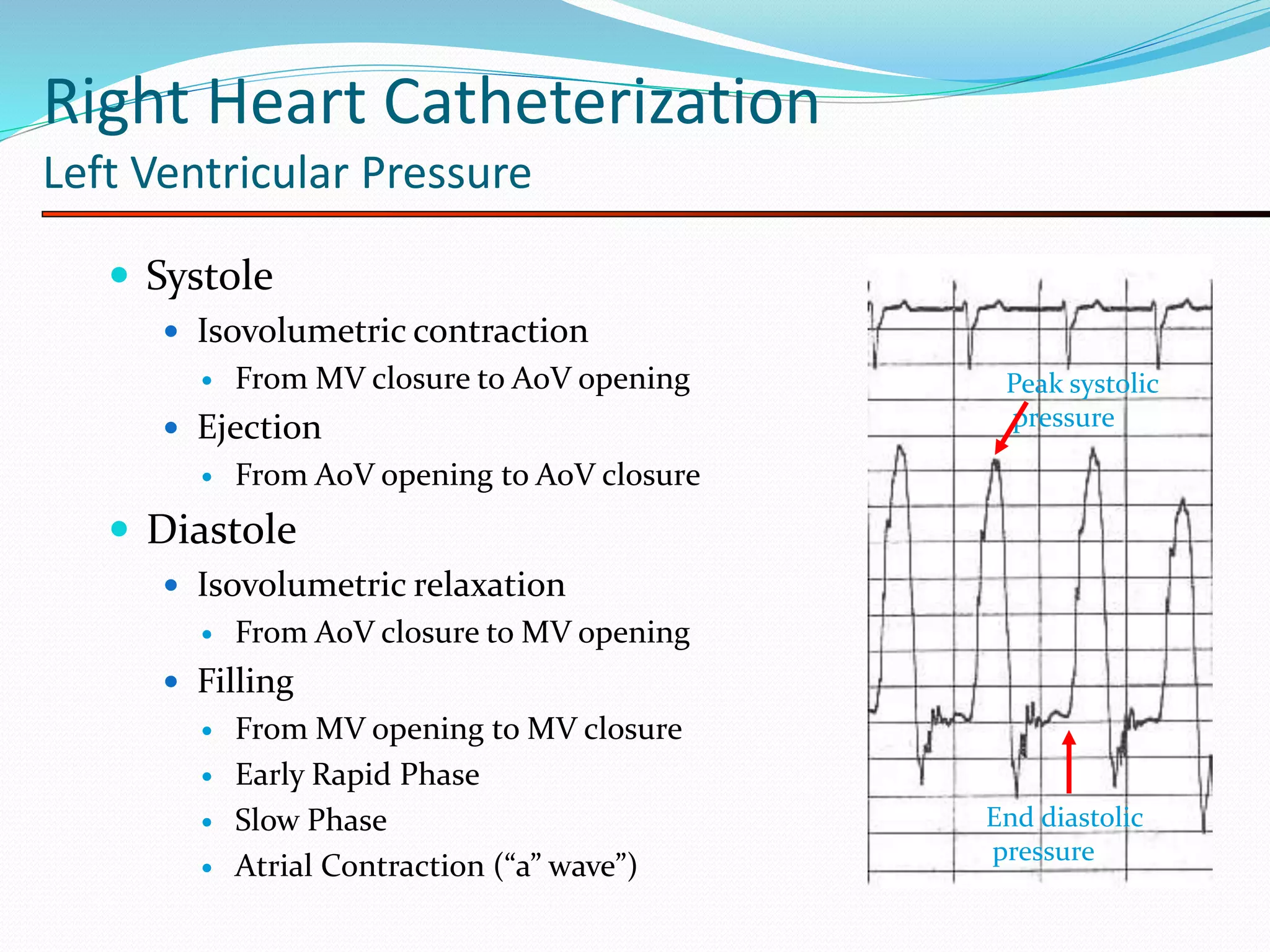
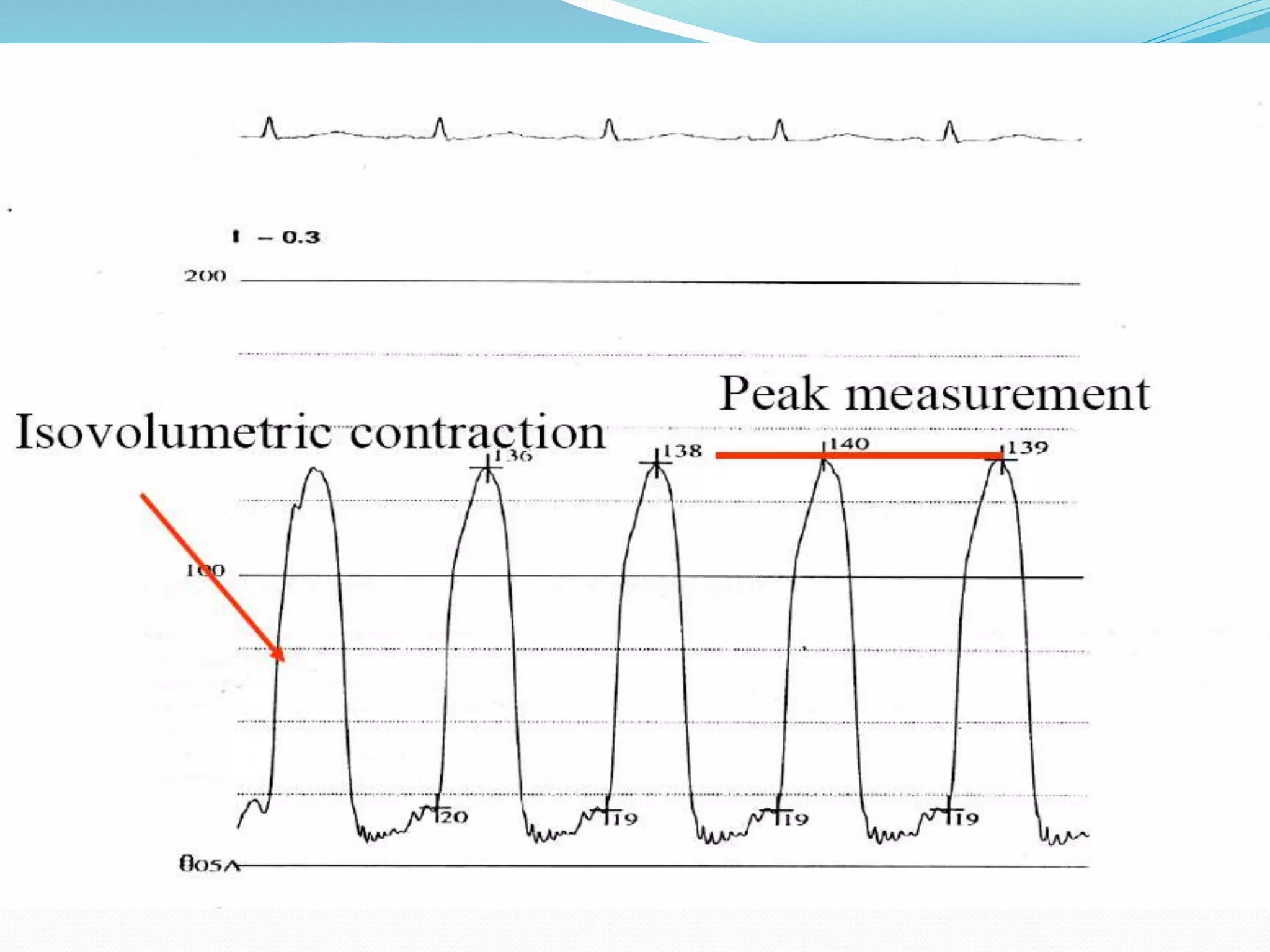



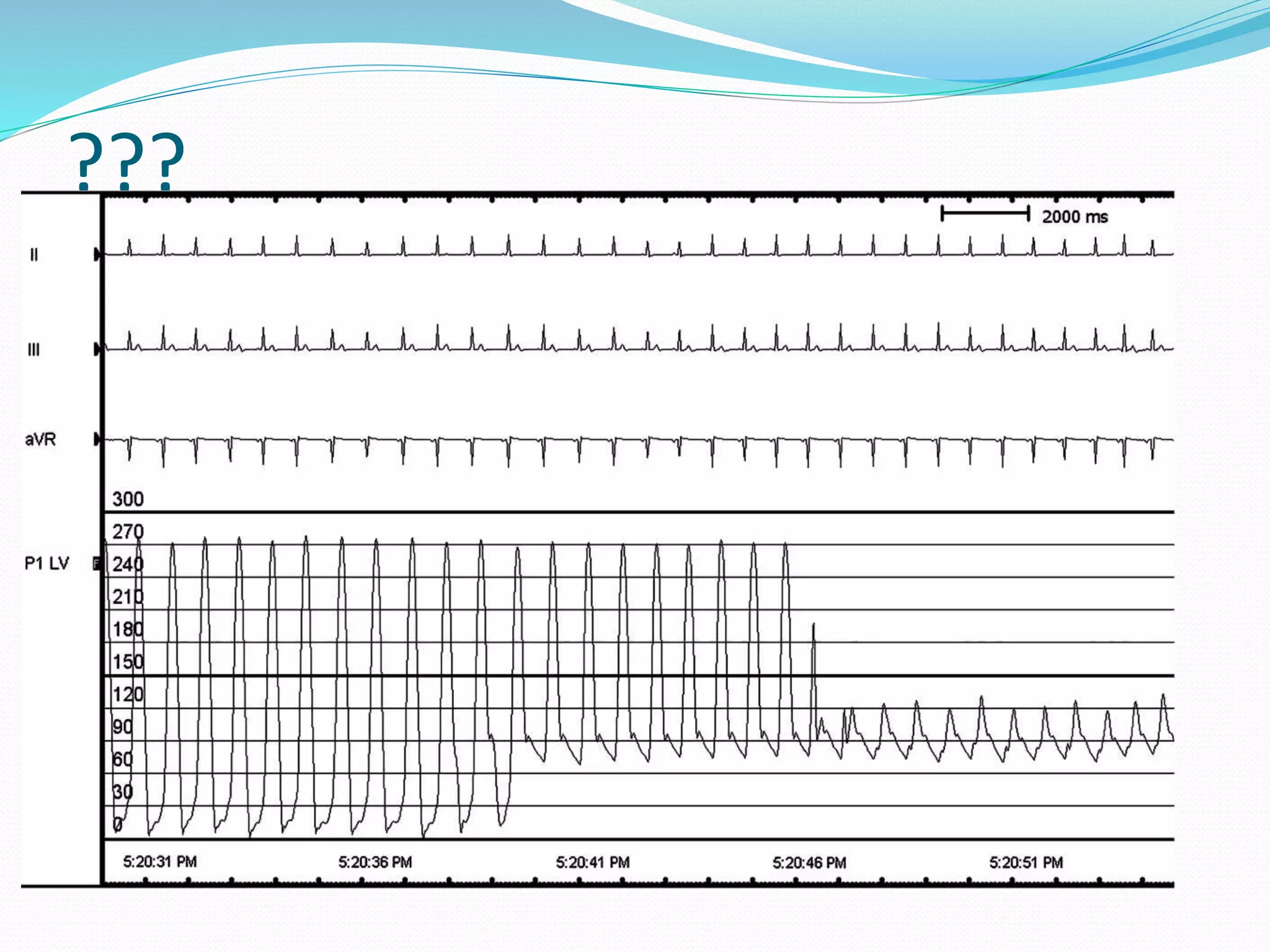


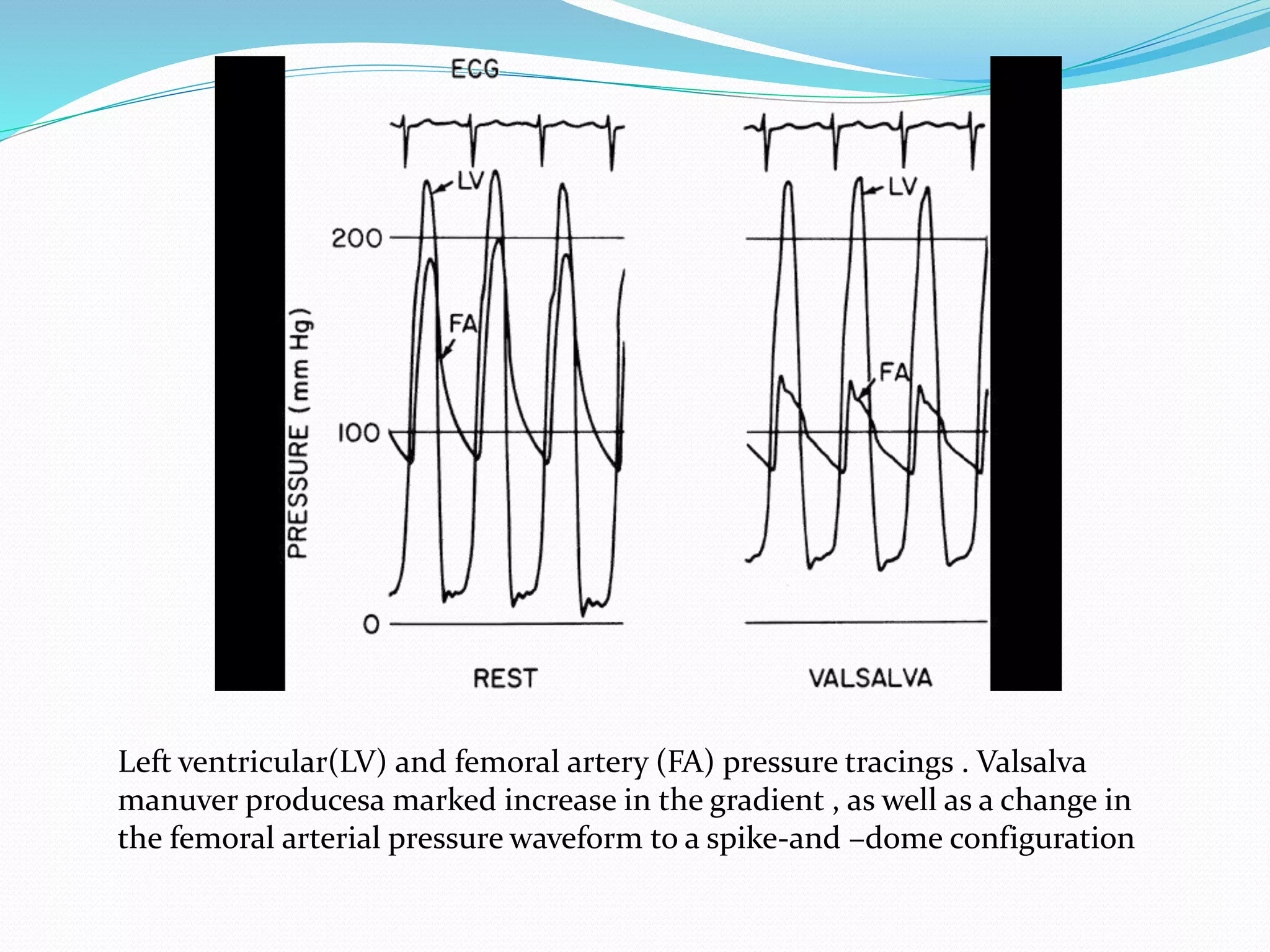

















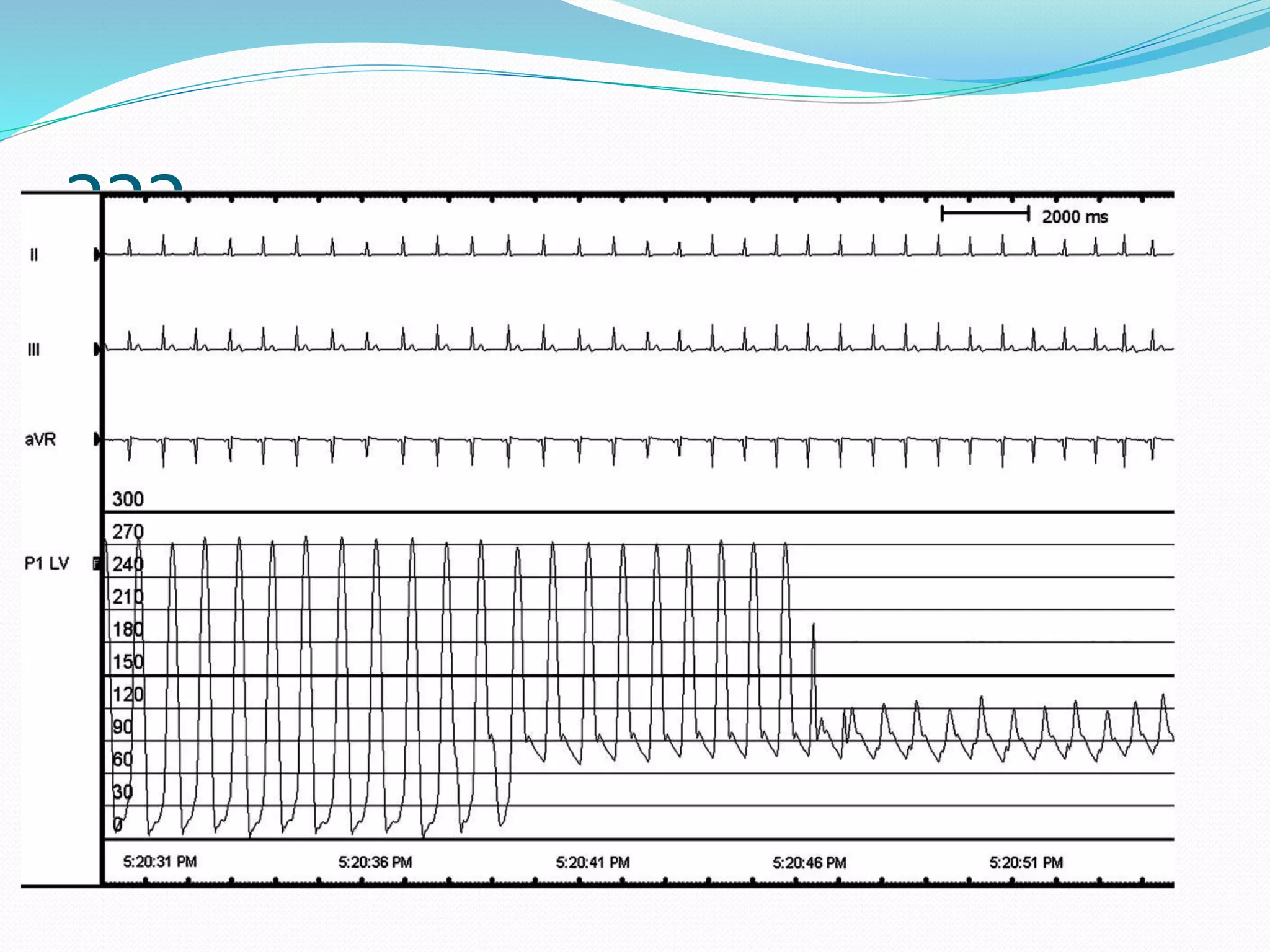


























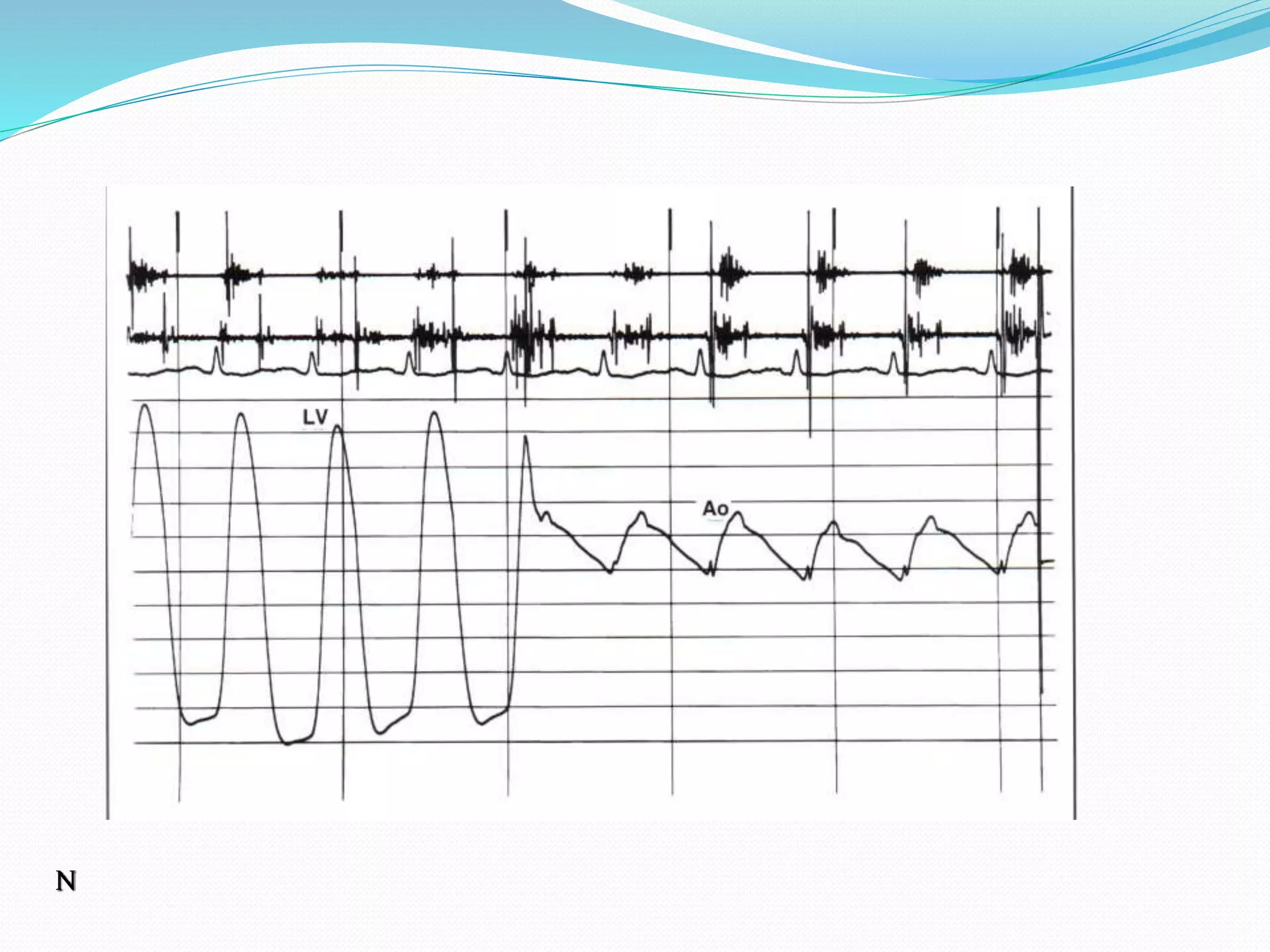



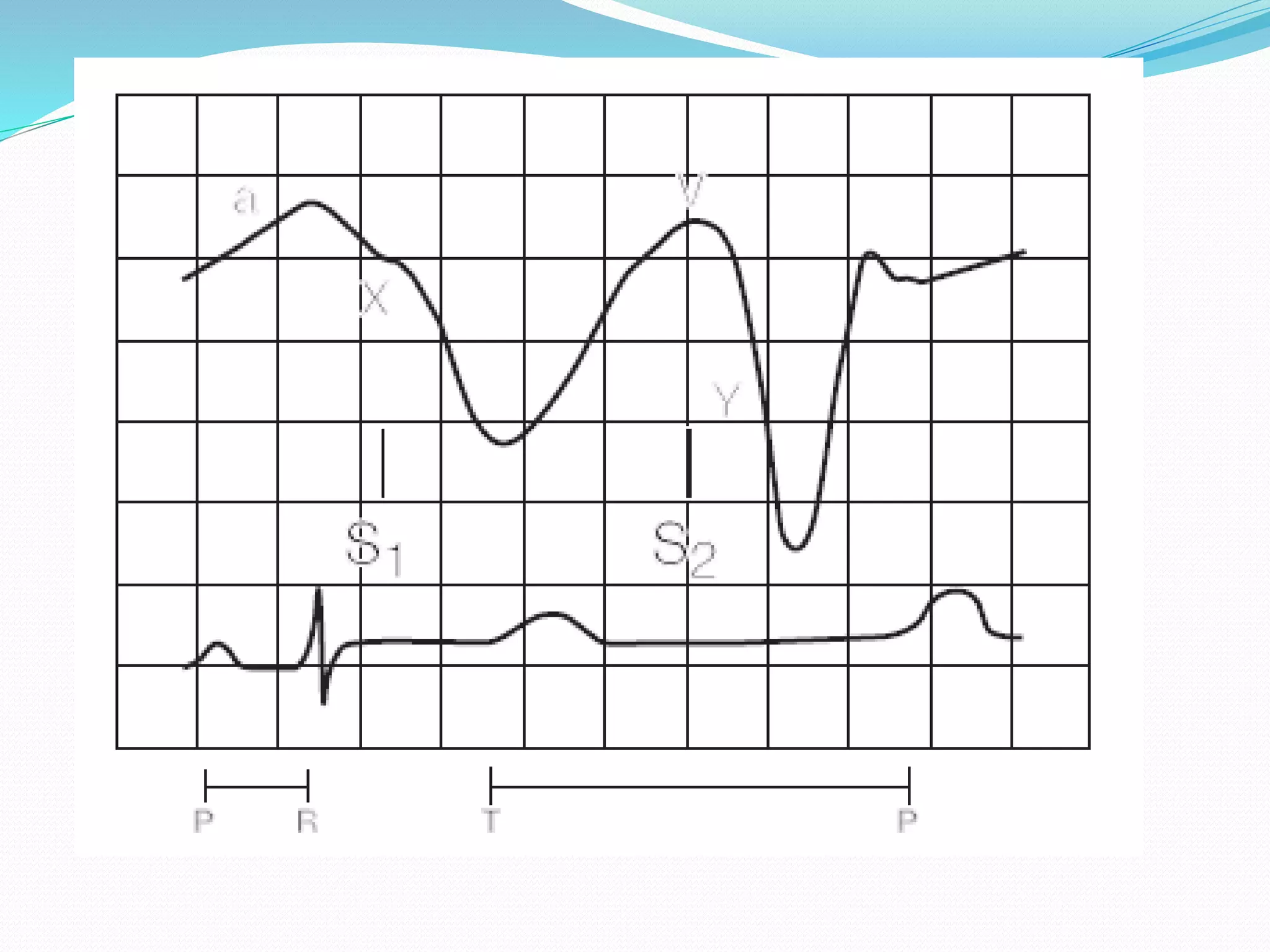


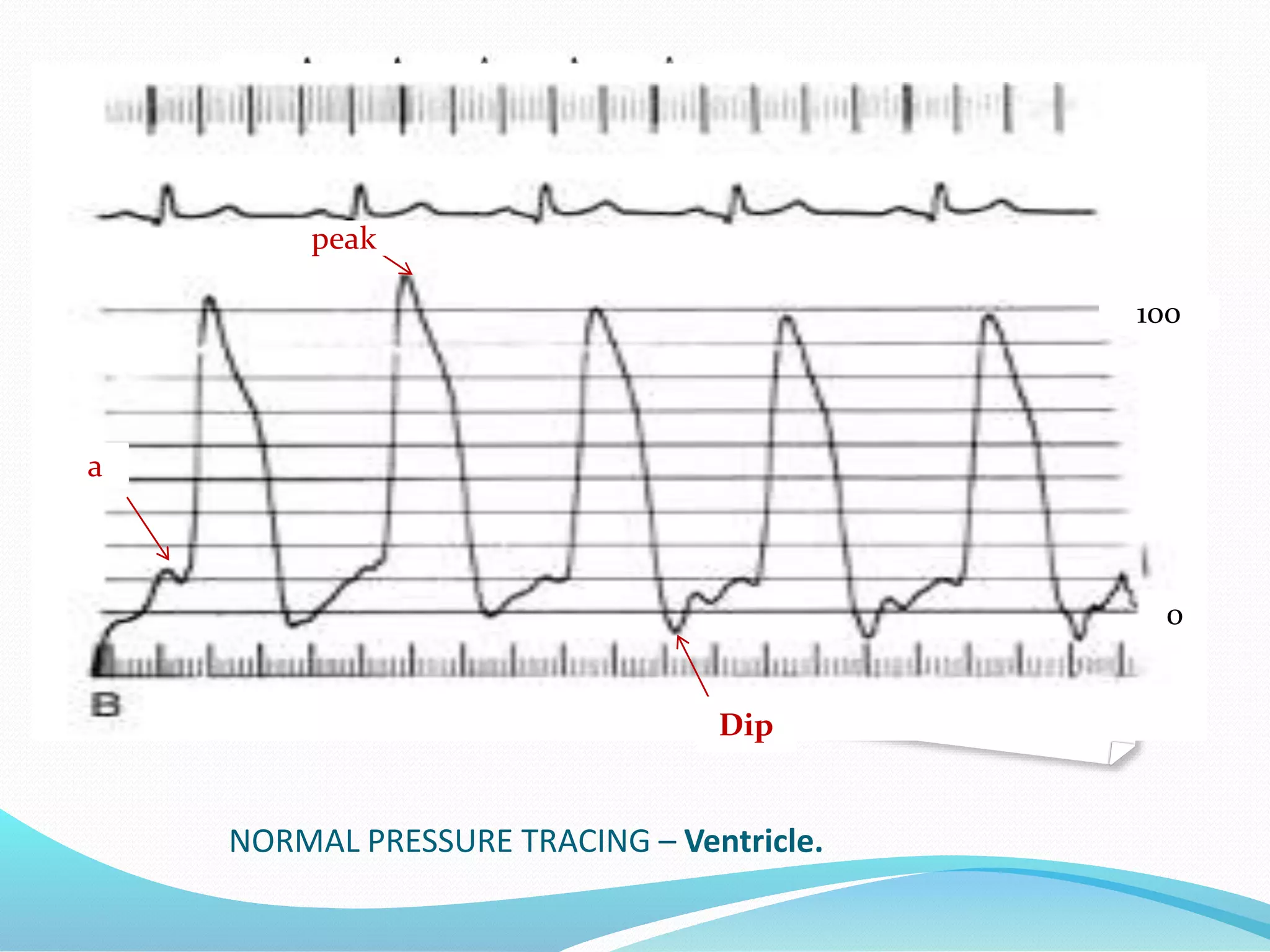











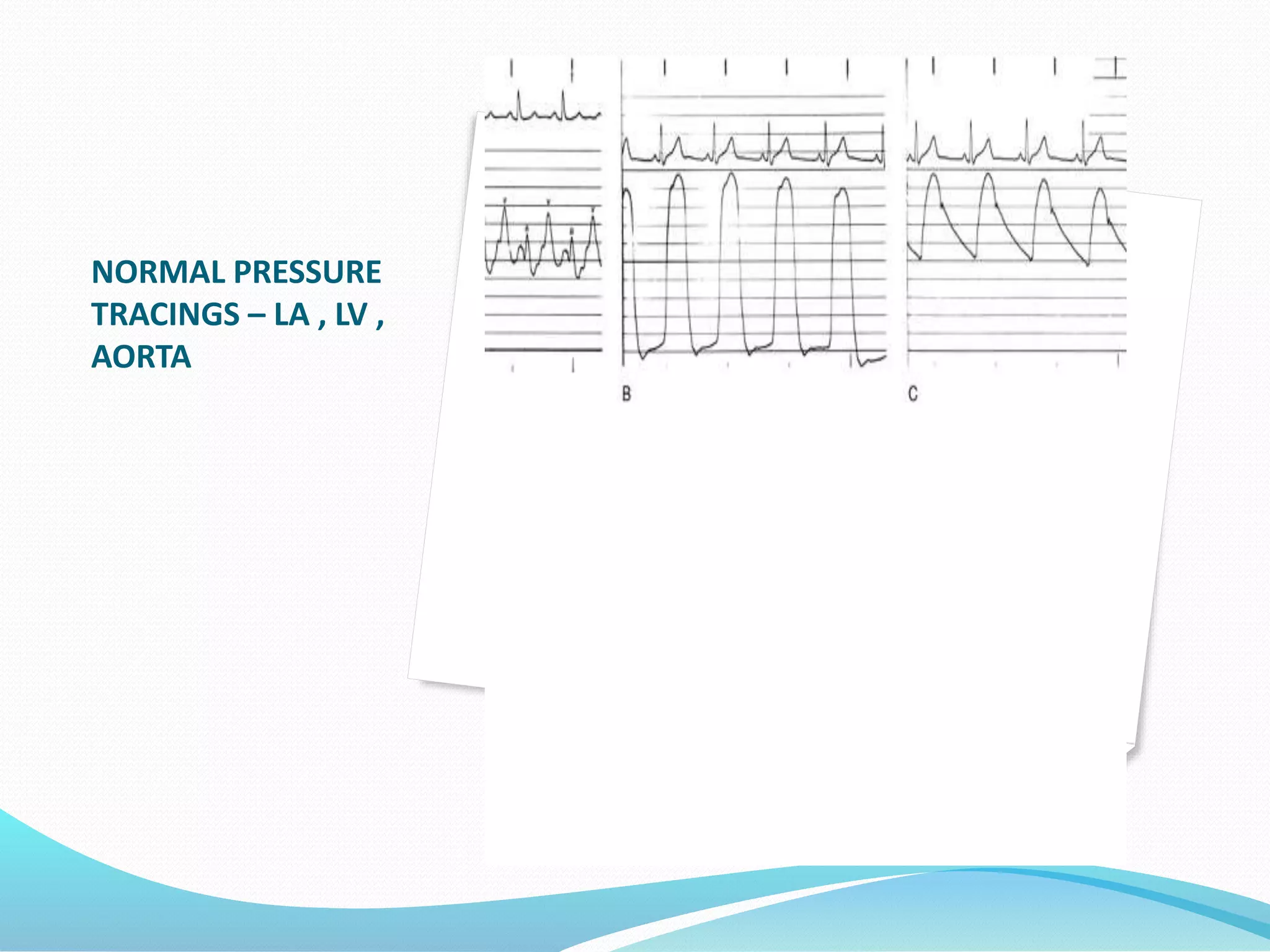



The document discusses left ventricular pressure tracings and their components during systole and diastole. It also discusses simultaneous pressure tracings from the left ventricle and aorta in a patient with aortic stenosis that show a fixed aortic obstruction. Finally, it examines left ventricular and left brachial artery pressure tracings in a patient with hypertrophic cardiomyopathy that show an increased gradient and spike-and-dome configuration in the arterial pressure waveform following an extrasystolic beat.























































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)











