Downloaded 26 times



![EpidemiologyEpidemiology TriadTriad
1. Agent: virulence
2. Host: Genetic susceptibility[3-5%]
3. Environment: Challenged socioeconomic](https://image.slidesharecdn.com/2arfrhd-160702152048/85/2-arf-amp-rhd-5-320.jpg)

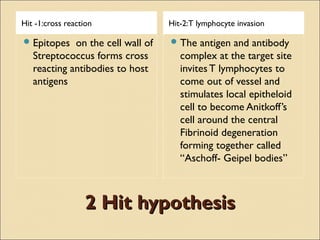
![(Modified from Parry E, Godfrey R, Mabey D, Gill G [eds]: Principles(Modified from Parry E, Godfrey R, Mabey D, Gill G [eds]: Principles
of Medicine in Africa. 3rd ed. Cambridge, Cambridge University Press,of Medicine in Africa. 3rd ed. Cambridge, Cambridge University Press,
2004, p 861.)2004, p 861.)
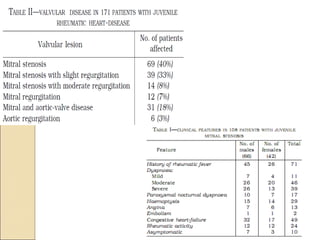
4 patterns RF in 150 years.
◦
A- Preantibiotic fall in the incidence of
ARF of industrialized countries
◦ B-Persistent high incidence RF
[Africa and south Asia].
◦ C-Postantibiotic fall in the incidence of
rheumatic fever in countries that
instituted comprehensive programs for
primary and secondary prevention of
rheumatic fever, such as Cuba, Costa
Rica, Martinique, and Guadeloupe.
◦ D-Fall and rise in the incidence of
rheumatic fever in the formerly Soviet
Republics of Central Asia.](https://image.slidesharecdn.com/2arfrhd-160702152048/85/2-arf-amp-rhd-7-320.jpg)



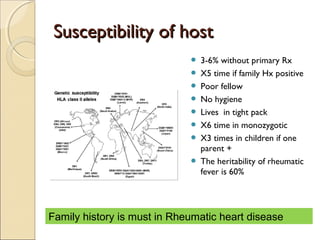
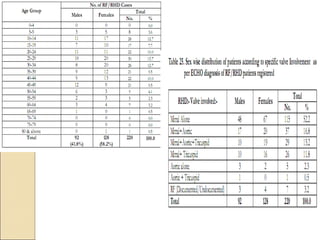
![PhotomicrographPhotomicrograph
Aschoff nodule of acute
rheumatic fever. The nodule is
composed of Anitschkow cells;
these have clear nuclei with a
central bar of chromatin, said to
resemble a caterpillar. There is a
central area of fibrin. This central
necrosis is further surrounded by
a mononuclear cell infiltrate.
Myocardial fibres adjacent to the
Aschoff body are undergoing
Fibrinoid necrosis. (Sebire NJ,
Ashworth M, Malone M, Jacques TS
[eds]: Diagnostic Pediatric Surgical
Pathology. Churchill Livingstone,
United Kingdom, 2010.)](https://image.slidesharecdn.com/2arfrhd-160702152048/85/2-arf-amp-rhd-13-320.jpg)































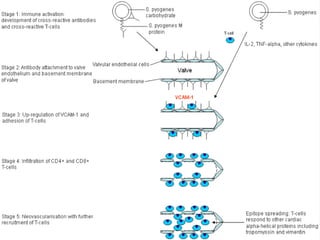





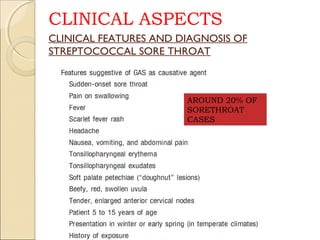

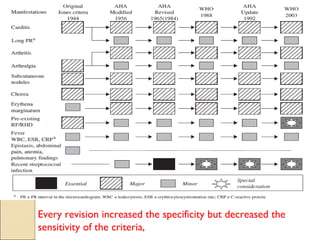







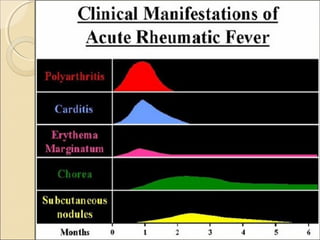

















































































This document discusses prevalence and incidence of acute rheumatic fever (ARF) and rheumatic heart disease (RHD) in India. It covers the molecular mimicry theory of how group A streptococcal pharyngitis can trigger an autoimmune response attacking the heart and other tissues. Host genetic factors play a role in susceptibility. Clinical manifestations of ARF include arthritis, carditis, chorea, and subcutaneous nodules. Echocardiography is important for diagnosing carditis. RHD remains a major cause of cardiovascular disease in India. Prevention requires prompt treatment of streptococcal infections.















































![Acute Rheumatic Fever – An Update[6704].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/acuterheumaticfeveranupdate6704-250603154932-9410381d-thumbnail.jpg?width=640&height=640&fit=bounds)




















































