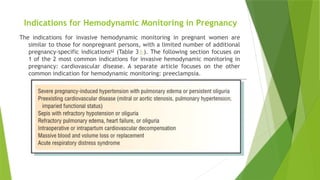
Indications for HemodynamicMonitoring in Pregnancy
The indications for invasive hemodynamic monitoring in pregnant women are
similar to those for nonpregnant persons, with a limited number of additional
pregnancy-specific indications62
(Table 3⇓). The following section focuses on
1 of the 2 most common indications for invasive hemodynamic monitoring in
pregnancy: cardiovascular disease. A separate article focuses on the other
common indication for hemodynamic monitoring: preeclampsia.
3.
Cardiovascular Disease
Althougha relatively small number of pregnancies (1%–2%) involve women
with cardiac disease, cardiovascular disease is the leading cause of indirect
maternal death during pregnancy.63
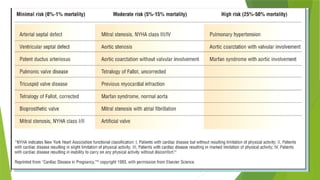
The risk of morbidity and mortality with cardiovascular disease depends on
the type of disease, the presence of pulmonary hypertension or cyanosis,
ventricular function, functional capacity, and history of cardiac surgery.63,66
Maternal mortality increases as the New York Heart Association functional
class increases (Table 4⇓).
5.
Use ofa pulmonary catheter is recommended only when
measurements of pressure and cardiac output of the left
side of the heart are required to guide therapy, for
example, in patients with complicated mitral or aortic
stenosis or pulmonary hypertension or patients with
impaired functional status (eg, New York Heart Association
functional class III or IV).62,66–
,70
However, use of a pulmonary artery catheter is not
generally recommended for patients with right ventricular
outflow obstruction, low pulmonary artery pressure, or
right-to-left shunt.
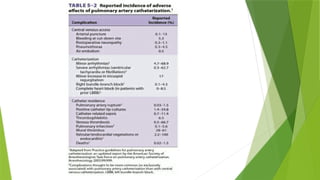
Additionally, the risk-to-benefit ratio of pulmonary artery
catheterization should be weighed in conditions associated
with an increased prevalence of catheter-related
complications (eg, Eisenmenger syndrome).71,72
6.
Cardiovascular
Monitoring
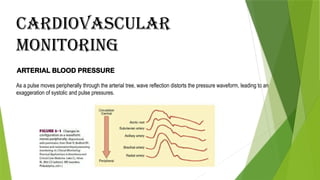
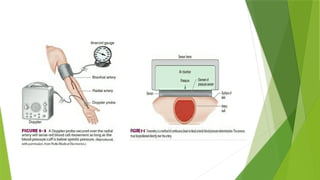
ARTERIAL BLOOD PRESSURE
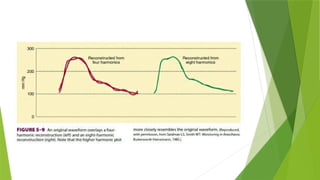
Asa pulse moves peripherally through the arterial tree, wave reflection distorts the pressure waveform, leading to an
exaggeration of systolic and pulse pressures.
7.
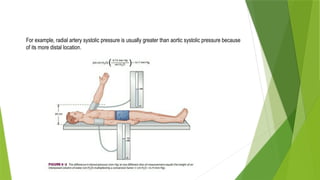
For example, radialartery systolic pressure is usually greater than aortic systolic pressure because
of its more distal location.
8.
1. Noninvasive ArterialBlood Pressure Monitoring
Indications : The use of any anesthetic, no matter how “trivial,” is an indication
for arterial blood pressure measurement.
Contra Indications : Although some method of blood pressure measurement is mandatory,
techniques that rely on a blood pressure cuff are best
avoided in extremities with vascular abnormalities (eg,
dialysis shunts) or with intravenous lines.
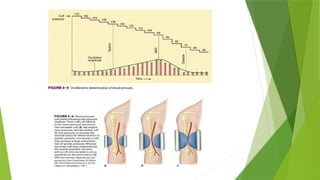
Technique & Complications :
a. Palpations
b. Doppler Probe
c. Auscultations
d. Oscillometry
e. Arterial Tonometri
11.
2. Invasive ArterialBlood Pressure Monitoring
Indications : Induced current or anticipated hypotension or wide blood
pressure deviations, end-organ disease
necessitating precise beat-to-beat blood pressure
regulation, and the need for multiple arterial blood gas
measurements.
Contra Indications : Should be avoided in smaller end arteries with inadequate collateral
blood flow or in extremities where
there is a suspicion of preexisting
vascular insufficiency
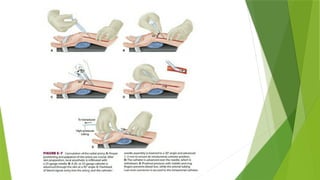
Selection of Artery for Cannulation :
a. Radial artery
b. Ulnar artery
c. Brachial artery
d. Femoral artery
e. Dorsalis pedis and posterior tibial arteries
f. Axillary artery
12.
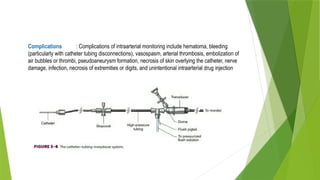
Complications : Complicationsof intraarterial monitoring include hematoma, bleeding
(particularly with catheter tubing disconnections), vasospasm, arterial thrombosis, embolization of
air bubbles or thrombi, pseudoaneurysm formation, necrosis of skin overlying the catheter, nerve
damage, infection, necrosis of extremities or digits, and unintentional intraarterial drug injection
15.
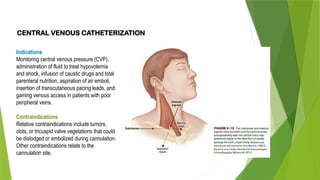
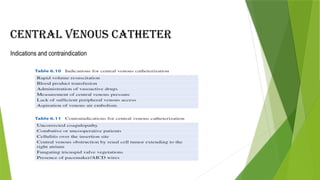
CENTRAL VENOUS CATHETERIZATION
Indications
Monitoringcentral venous pressure (CVP),
administration of fluid to treat hypovolemia
and shock, infusion of caustic drugs and total
parenteral nutrition, aspiration of air emboli,
insertion of transcutaneous pacing leads, and
gaining venous access in patients with poor
peripheral veins.
Contraindications
Relative contraindications include tumors,
clots, or tricuspid valve vegetations that could
be dislodged or embolized during cannulation.
Other contraindications relate to the
cannulation site.
16.
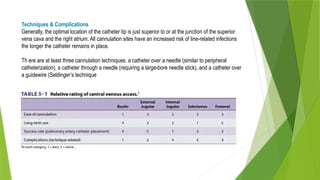
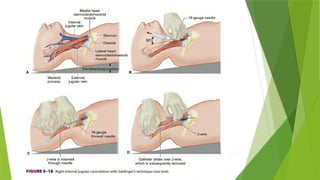
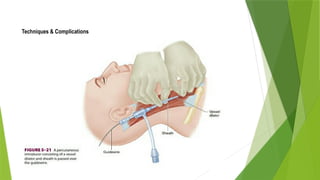
Techniques & Complications
Generally,the optimal location of the catheter tip is just superior to or at the junction of the superior
vena cava and the right atrium. All cannulation sites have an increased risk of line-related infections
the longer the catheter remains in place.
Th ere are at least three cannulation techniques: a catheter over a needle (similar to peripheral
catheterization), a catheter through a needle (requiring a large-bore needle stick), and a catheter over
a guidewire (Seldinger’s technique
18.
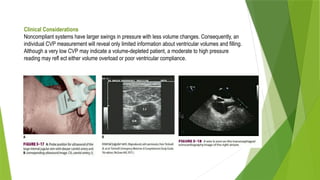
Clinical Considerations
Noncompliant systemshave larger swings in pressure with less volume changes. Consequently, an
individual CVP measurement will reveal only limited information about ventricular volumes and filling.
Although a very low CVP may indicate a volume-depleted patient, a moderate to high pressure
reading may refl ect either volume overload or poor ventricular compliance.
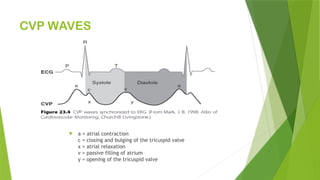
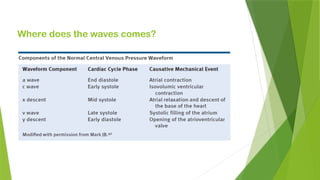
a =atrial contraction
c = closing and bulging of the tricuspid valve
x = atrial relaxation
v = passive filling of atrium
y = opening of the tricuspid valve
CVP WAVES
CAUSES OF RAISEDCVP
• Right ventricular failure
• Tricuspid stenosis or regurgitation
• Pericardial effusion or constrictive pericarditis
• Superior vena caval obstruction
• Fluid overload
• Hyperdynamic circulation
• High PEEP settings
23.
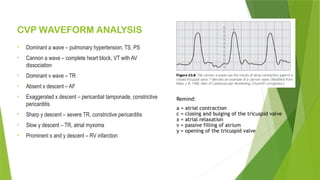
CVP WAVEFORM ANALYSIS
•Dominant a wave – pulmonary hypertension, TS, PS
• Cannon a wave – complete heart block, VT with AV
dissociation
• Dominant v wave – TR
• Absent x descent – AF
• Exaggerated x descent – pericardial tamponade, constrictive
pericarditis
• Sharp y descent – severe TR, constrictive pericarditis
• Slow y descent – TR, atrial myxoma
• Prominent x and y descent – RV infarction
Remind:
a = atrial contraction
c = closing and bulging of the tricuspid valve
x = atrial relaxation
v = passive filling of atrium
y = opening of the tricuspid valve
24.
PITFALL
However, CVPtrends can be useful if measurements are made with consistent techniques and
absent LV dysfunction, severe mitral regurgitation, and pulmonary hypertension. As with most
clinical data, they should be considered alongside all other clinical and laboratory indicators of
perfusion.
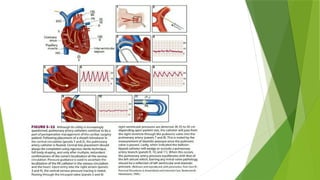
Respiratory variation-based indicators: during spontaneous breathing, blood pressure normally
decreases (<5 mm Hg) during the negative intrathoracic pressure period of inspiration.
Exaggerated decreases as seen in constrictive pericarditis and severe asthma exacerbation are
termed “pulsus paradoxus.” The reverse is seen during mechanical ventilation, where cyclic
changes in intrathoracic pressure and volume cause cyclic changes in LV preload and, therefore, in
stroke volume (SV) and blood pressure.
Pulse pressure variation physiology: physiologic changes during mechanical ventilation are
complex; however, major changes during positive pressure (i.e., inspiration) include: (1) decreased
venous return, which within several beats of end inspiration results in decreased LV preload and
CO; (2) increased RV afterload secondary to increased alveolar pressure transmitted to the
pulmonary capillaries; (3) initial increased LV preload secondary to the squeezing out
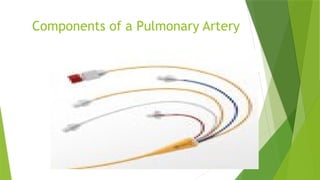
Components of Swan-Ganz[con’t]
Normally has four[4] ports
Proximal port – [Blue] used to measure central
venous pressure/RAP and injectate port for
measurement of cardiac output
Distal port – [Yellow] used to measure pulmonary
artery pressure
Balloon port – [Red] used to determine pulmonary
wedge pressure;1.5 special syringe is connected
Infusion port – [White] used for fluid infusion
29.
Components of theMonitoring
System
Bedside monitor – amplifier is located inside. The amplifier increases the size
of signal
Transducer – changes the mechanical energy or pressures of pulse into
electrical energy; should be level with the phlebostatic axis[ you can estimate
this by intersecting lines from the 4th
ICS,mid axillary line
Recorder – please record information
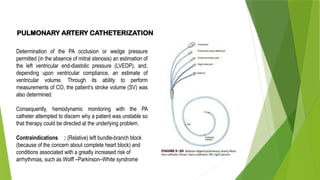
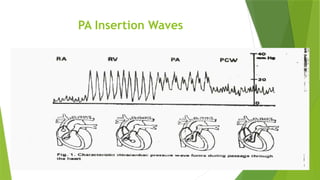
PULMONARY ARTERY CATHETERIZATION
Determinationof the PA occlusion or wedge pressure
permitted (in the absence of mitral stenosis) an estimation of
the left ventricular end-diastolic pressure (LVEDP), and,
depending upon ventricular compliance, an estimate of
ventricular volume. Through its ability to perform
measurements of CO, the patient’s stroke volume (SV) was
also determined.
Consequently, hemodynamic monitoring with the PA
catheter attempted to discern why a patient was unstable so
that therapy could be directed at the underlying problem.
Contraindications : (Relative) left bundle-branch block
(because of the concern about complete heart block) and
conditions associated with a greatly increased risk of
arrhythmias, such as Wolff –Parkinson–White syndrome
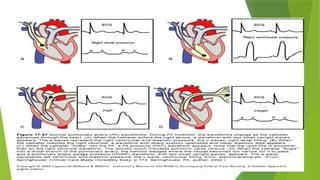
Clinical Considerations
Starling demonstratedthe relationship between left ventricular function and left ventricular
enddiastolic muscle fiber length, which is usually proportionate to end-diastolic volume. If
compliance is not abnormally decreased (eg, by myocardial ischemia, overload, ventricular
hypertrophy, or pericardial tamponade), LVEDP should reflect fiber length. In the presence of a
normal mitral valve, left atrial pressure approaches left ventricular pressure during diastolic filling.
The left atrium connects with the right side of the heart through the pulmonary vasculature. The
distal lumen of a correctly wedged PA catheter is isolated from rightsided pressures by balloon
inflation.


![Components of Swan-Ganz [con’t]
Normally has four[4] ports
Proximal port – [Blue] used to measure central
venous pressure/RAP and injectate port for
measurement of cardiac output
Distal port – [Yellow] used to measure pulmonary
artery pressure
Balloon port – [Red] used to determine pulmonary
wedge pressure;1.5 special syringe is connected
Infusion port – [White] used for fluid infusion](https://image.slidesharecdn.com/monitoringinvasifanestesia-250809034515-f2a22ca5/85/Monitoring-Invasif-Anesthesai-in-java-27-320.jpg)


































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)















