Downloaded 243 times
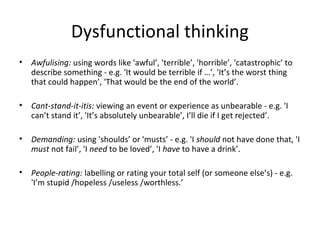
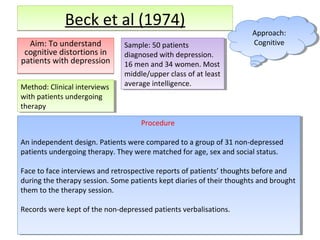
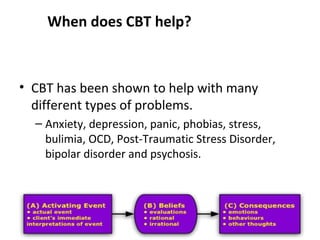


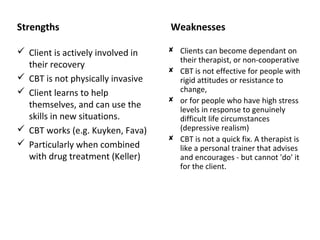

The cognitive perspective assumes that: - Individuals with mental disorders have distorted and irrational thinking that can cause maladaptive behavior. - It is one's thoughts about a problem, not the problem itself, that causes the mental disorder. - People can overcome mental disorders by learning to use more rational and adaptive cognitions.
























































![Anxiety disorders unit intervention[2]](https://cdn.slidesharecdn.com/ss_thumbnails/anxietydisordersunitintervention2-111028091300-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
