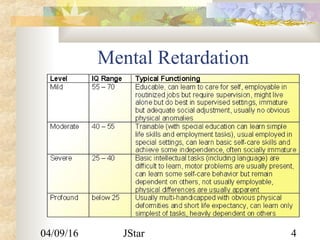
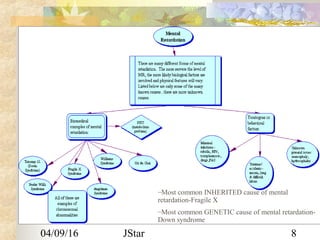
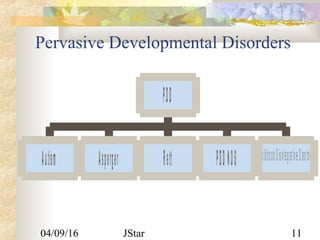
This document provides information on several childhood psychiatric disorders and conditions. It discusses mental retardation and the different classifications based on IQ. It also covers pervasive developmental disorders like autism and Asperger's disorder. Learning disorders and disruptive disorders like oppositional defiant disorder and conduct disorder are explained. The document also summarizes attention deficit hyperactivity disorder, movement disorders, encopresis, enuresis, and toilet training.