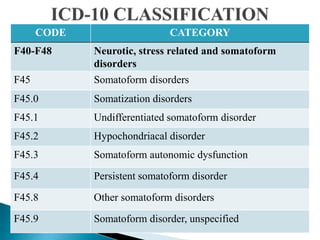
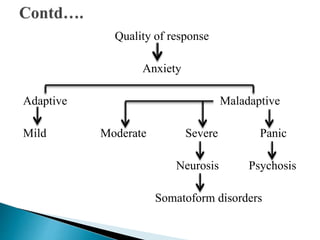





This document discusses somatoform disorders. It begins by defining somatoform disorders as mental illnesses characterized by physical symptoms that cannot be fully explained medically and cause impairment. Key points include: somatoform disorders involve the presentation of physical complaints due to psychological factors; they are characterized by multiple somatic complaints and persistent healthcare seeking despite reassurance; and common types include somatization disorder, conversion disorder, and hypochondriasis. Treatment involves identifying and addressing the underlying psychological causes through cognitive behavioral therapy and other approaches.
























































![Revised Topic- Schizophrenia [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/schizophreniaautosaved-250310073514-5d1607b2-thumbnail.jpg?width=640&height=640&fit=bounds)





![Revised -ppt of child psychiatric problems [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/pptofchildpsychiatricproblemsautosaved-240926091227-d0592556-thumbnail.jpg?width=640&height=640&fit=bounds)























